
A comprehensive review of chalazions and chalazia with a depiction of the many different faces of chalazia
Dr. BCK Patel MD, FRCS
For family practice doctors, physicians, oculoplastic surgeons, ophthalmologists, residents and fellows
What is a chalazion?

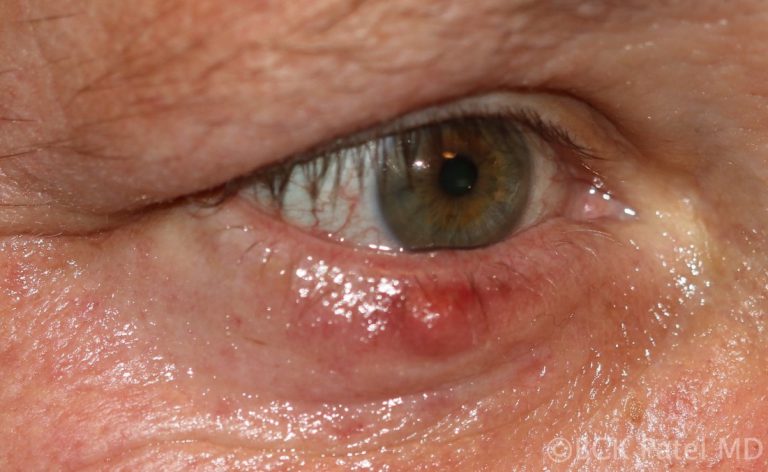
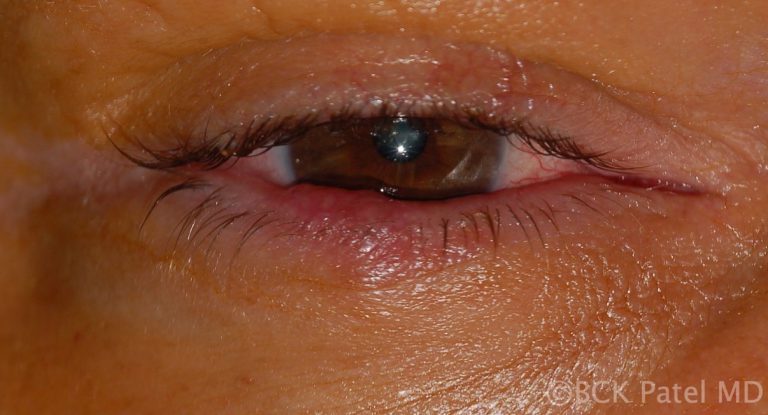
A chalazion is initially a painless mass that develops on the eyelid. It is caused by a blockage of the Meibomian gland. The blocked gland allows the contents (lipogranulomatous material) to expand and will eventually allow the material to spread into the surrounding tissues, causing local inflammation.
Initially, the chalazia are soft or rubbery but go on to become firm. Inflammation or secondary infection will lead to tenderness of the lesions. Does an initial infection of the Meibomian gland cause a chalazion to develop or is it a blocked Meibomian gland that secondarily becomes inflamed and can become infected? The exact sequence is probably both of the above in different lesions.

Etymology of the word “Chalazion”
“Khalaza” is a Greek word meaning a “small knot”. The diminutive of “khalaza” is “khalazion”. Therefore the singular is “chalazion” and the plural is “chalazia” or “chalazions.

Synonyms
Tarsal cyst, Meibomian cyst, External hordeolum (the word “hordeolum: is from the Latin “hordeolus” which stands for “barley” and was used because of the resemblance of the anterior chalazion to a grain of barley, Internal hordeolum


Increased risk of developing chalazia
- Smoking
- Blepharitis
- Dry eye syndrome
- Eyelid skin dermatitis
- Acne rosacea
- History of allergic skin conditions
- Gastritis and irritable bowel syndrome (although the exact correlation is unknown)
Natural history of a chalazion
The initial inciting factor is blockage of a Meibomian gland. This causes the sebaceous material that is within the meibomian gland to expand. This results in a painless swelling, which is called a chalazion. Initially, the lesions are painless and expand slowly. Local tenderness occurs when there is spread of the sebaceous material to the surrounding tissues leading to local inflammation, or if there is a secondary infection which results in increased tenderness.
Untreated, chalazia can increase in size and become quite firm although most will burst through to the surface (skin) or through the conjunctiva and will resolve slowly but surely.
Chalazia may occur in childhood and in adults, often in the 30 – 50 age group. Predisposing factors include conditions like underlying blepharitis and acne rosacea. The use of makeup and the wearing of contact lenses does not increase the incidence of chalazia.
Recently, with Covid, it has become apparent that the wearing of masks may lead to a drying effect on the eyelid margins with secondary blockage of the Meibomian glands. We have seen a significant increase in the incidence of chalazia during the Covid years 2020-2023.
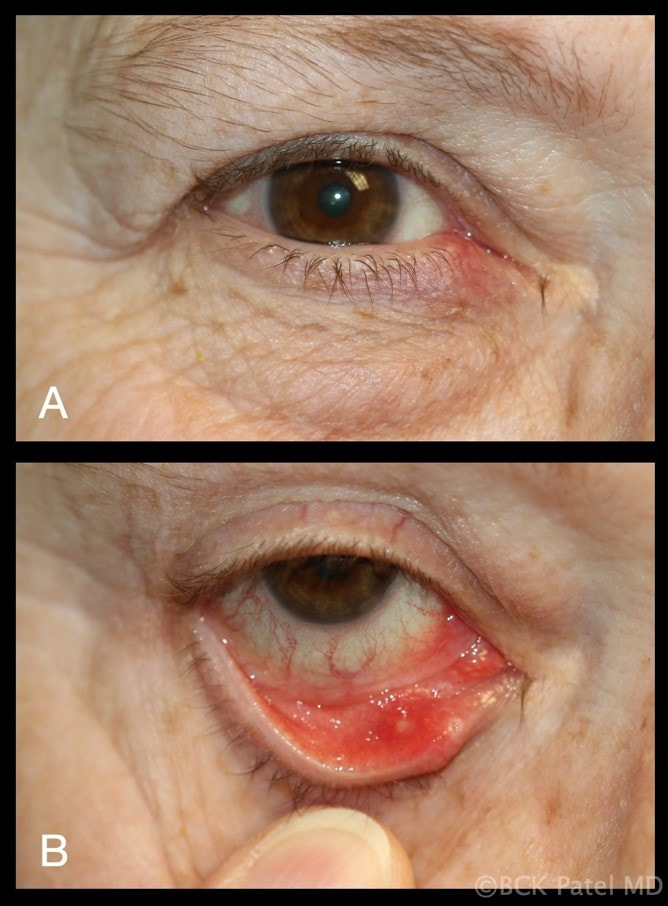
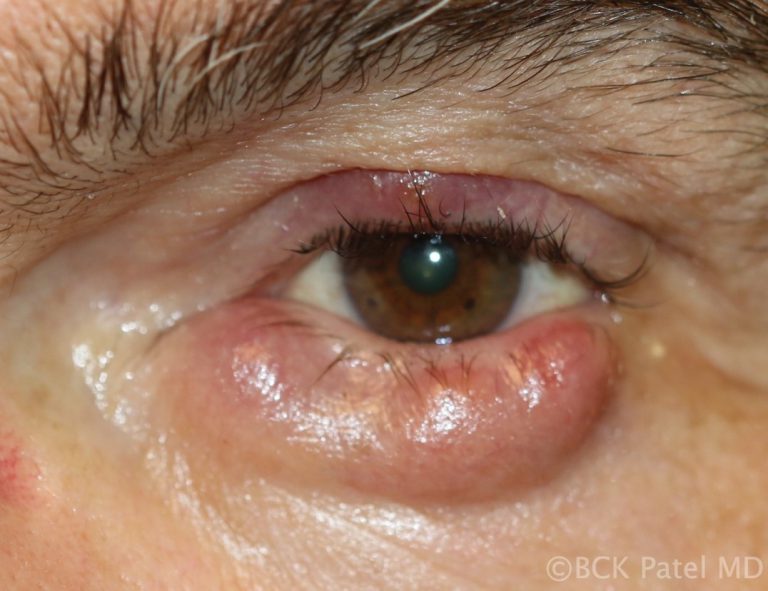
A large chalazion on the upper eyelid may cause a mechanical ptosis. The change in the curvature of the eyelid and also the pressure on the cornea can make it difficult to wear contact lenses.
Lower eyelid chalazia can result in an ectropion with resultant epiphora (tearing). Secondary calcification may develop in the presence of chronic chalazia. Malignant transformation is extremely rare.

External Hordeolum
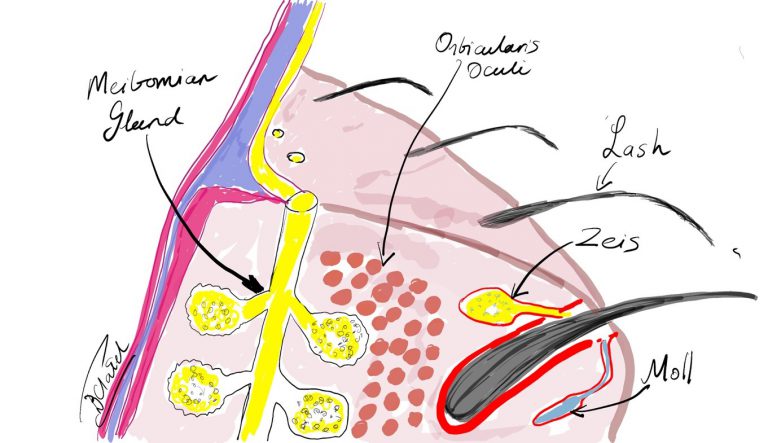
Infections of the glands of Zeis are called styes or external hordeolum. These sebaceous oil glands open into the eyelash follicles. The term external hordeolum has erroneously been used for a chalazion that becomes infected and erodes through the skin.

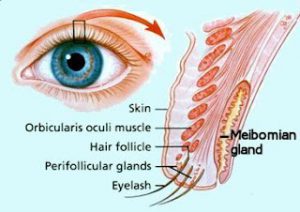
What are Meibomian Glands?
Meibomian glands ae glands within the tarsus of the upper and lower eyelids. There are 30 glands in the upper eyelid and about 25 glands in the lower eyelid. They are also called tarsal glands.

Meibomian glands produce an oily substance called meibum which is important in reducing the evaporation rate of tears in our tear film. These are exocrine glands: they have ducts that secrete their contents via ducts that open at the eyelid margin. They are also holocrine glands because the secretions result from lysis of the secretory glands, which causes them to release the oily substance into the Meibomian duct. Meibum not only reduces evaporation of the aqueous component of the tear film, but it also keeps the aqueous component from spilling over the edge of the eyelid by forming a film on the tear film and at the edge of the eyelid. Meibum further assists in allowing the eyelids to shut in an airtight manner.
Meibomian Glands: Etymology
Heinrich Meibom (1638 – 1700) was a German physician who studied in France, Germany, Italy and England. He went on to become a Professor of Medicine and also a Professor of History and Poetry. He wrote Latin poetry for which he was well known.

Differential Diagnosis of a Chalazion
- Stye
- Adenocarcinoma
- Sebaceous Gland Carcinoma
- Nodular basal cell carcinoma
- Schwannoma

Histopathology of Chalazia
Histopathology of the contents of a chalazion reveals a lipogranulomatous reaction with multinucleated giant cells, foamy macrophages, plasma cell, neutrophils and lymphocytes with lipid vacuoles.
Histopathology will show areas of clear spaces which do not stain with H&E staining because these are lipid droplets. Older lesions may manifest fibrosis
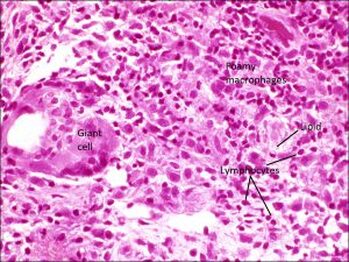
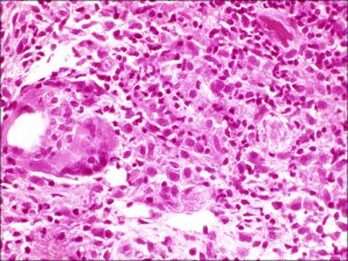
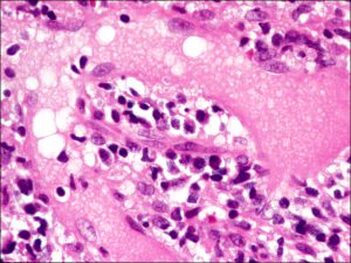
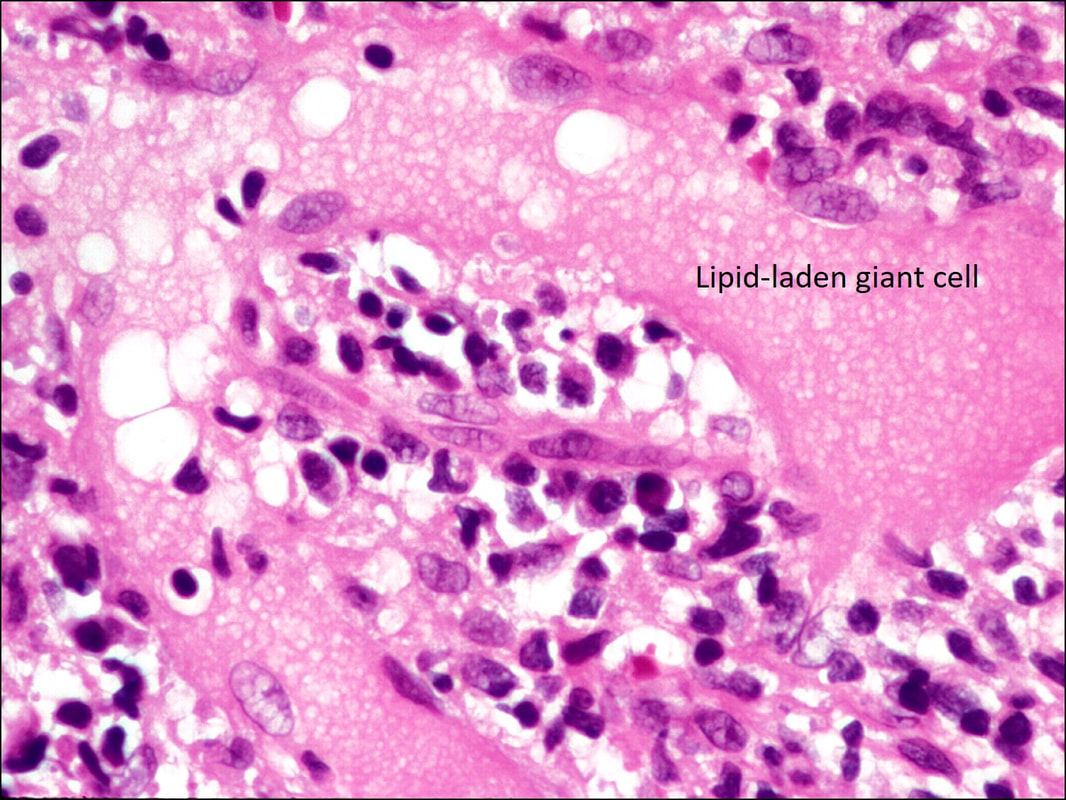
Histopathology courtesy of Prof. Nick Mamalis MD, MoranCore
How do you manage chalazia presenting acutely?



Patients may present with a non-tender bump on the upper or lower eyelid, in which case the lesion may cause distortion of the cornea which affects vision or may be cosmetically unacceptable. Larger lesions can cause pressure on the cornea with resultant astigmatism. Central chalazia can be in the line of sight and can also cause a mechanical ptosis interfering with the field of vision.
Management:
- Warm soaks ae applied to the lesion four to five times a day
- Topical antibiotic ointment or an antibiotic-steroid ointment is prescribed to be used three times a day to the lesion
- Heat may be applied to the lesions with heated rice-pods or even a microwaved potato!
- The important thing to remember is to apply pressure on the enlarged Meibomian gland: this pressure allows the contents to become softer and allows egress of the material from the Meibomian gland.
- Systemic antibiotics are usually not indicated for simple chalazia. These may be prescribed if there is local spread of inflammation into the eyelid with resulting preseptal cellulitis
- If the gland is inflamed, it is best to incize and drain the lesion via the conjunctival approach. If a chalazion is already erupting through the skin of the eyelids, it is reasonable to make the opening on the cutaneous side. See our videos which demonstrate the technique of incizing and draining chalazia. After incizing and draining chalazia, the patient is asked to continue warm soaks and apply the prescribed ointment three times a day for a week



Management of Chronic Chalazia


After a few weeks, chalazia can become firm and even nodular. If left untreated, these chalazia can take weeks to months to slowly resolve. As the mass effect is often a nuisance in the presence of chronic chalazia, we usually carry out incision and drainage of the lesions with local anesthetic injection and inject the firm remnant of the chalazion with dexamethasone 4% solution.
Whenever draining chalazia, the following points must be followed:
- Drainage is with vertical incisions on the conjunctival side of the tarsus unless the lesion is erupting through the skin of the eyelid
- Only make vertical incisions and not horizontal like some textbooks portray. And certainly do not create vertical and horizontal incisions and excize parts of the tarsus as some ophthalmic books illustrate. There is no reason to sacrifice the tarsal plate unless a biopsy is being obtained (see below)
- Beware of involvement of surrounding Meibomian glands. It is not uncommon to find other glands adjacent to the inflamed or blocked Meibomian gland to also be affected. They will also need draining. We frequently apply the two-finger pressure technique to chalazia that we drain to ensure that we also drain any surrounding inspissated glands

Chronic Meibomianitis
Patients with acne rosacea and chronic blepharitis can present with chronic meibomianitis with multiple glands being inflamed and varying number of chalazia. These patients will often present with recurring chalazia and will require topical tetracycline as well as management of the underlying condition. There may be a reduction of eyelashes even in the absence of malignancy. Treatment with intense pulsed light has been shown to improve acne rosacea and also inflammation of the eyelids.

Beware Chronic Chalazia in Older Patients or Recurring Chalazia
Chronic chalazia in older patients or recurrent multiple chalazia should alert the physician to perform a biopsy as sebaceous gland carcinomas can mimic chalazia. If the chalazion has a smooth yellow surface without discomfort, it is best to biopsy the lesion. Also look for any associated loss of eyelashes. Specimens should be submitted fresh to the ophthalmic pathologist for appropriate staining looking for evidence of sebaceous gland carcinoma

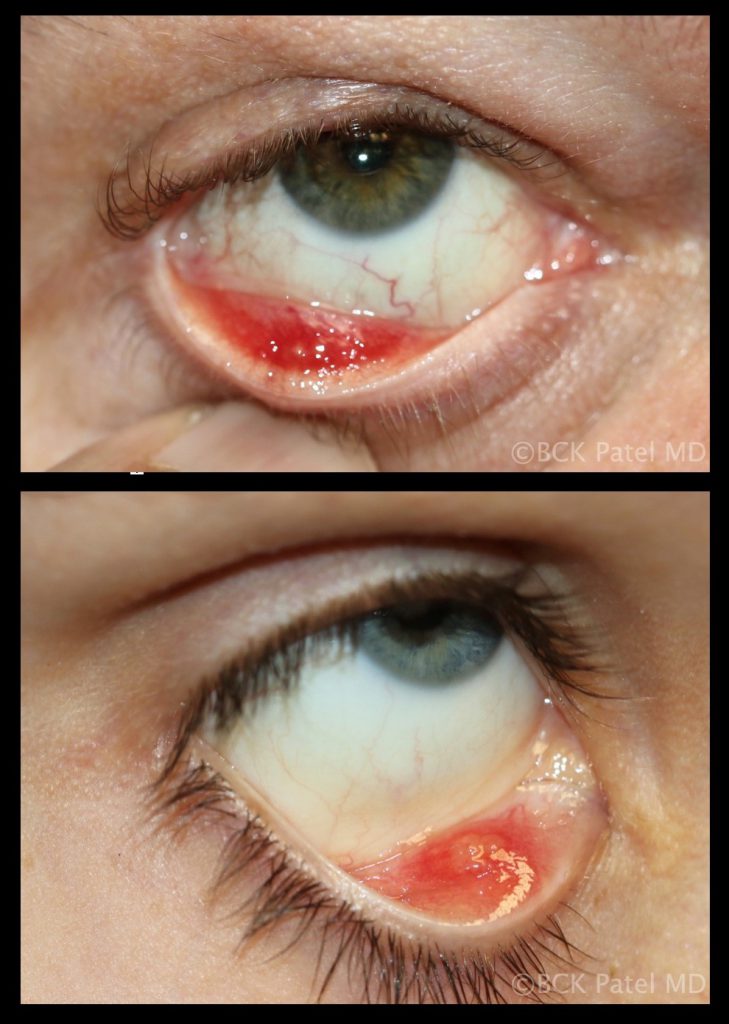
Chronic Chalazia with Pyogenic Granulomas

Chronic inflammation that bursts through the conjunctival surface can sometimes present with a pendulous inflammatory mass which is a pyogenic granuloma. These are removed surgically and the base scraped with a chalazion scoop and a steroid injection is administered

Chalazia with Secondary Cellulitis

Multiple chalazia, especially in children, can spread inflammation and secondary infection into the surrounding skin resulting in a preseptal cellulitis. Indeed, whenever preseptal cellulitis is seen in children, always palpate the eyelids to exclude the presence of inflamed chalazia. Once the underlying chalazia are properly treated, the cellulitis will resolve.


Multiple Chalazia
Multiple chalazia are seen in patients with chronic Meibomian gland disease, acne rosacea and chronic blepharitis. Multiple chalazia may also present in multiple eyelids and are thought to be hormonally related in females.


When should steroids be injected into chalazia?
50% of early soft chalazia will resolve just with an intralesional injection of a steroid like dexamethsone. When the lesion or lesions are firm and multiple, it is best to administer local anesthetic, perform an incision and curettage and then inject with a steroid.
Indications for Incision and Curettage


- Early soft chalazia can be incized and drained when the patient wants a quick resolution
- Chronically inflamed and tender chalazia should be incized and drained
- Recurrent chalazia should be incized and drained and biopsied if indicated
- Multiple chalazia are best injected with local anesthetic, drained and injected with steroids
How do you perform an incision and curettage of a chalazion?

Instruments
- Topical xylocaine drops or gel
- 11 Bard Parker blade
- 2% lidocaine with epinephrine on a 30 or 32 gauge needle
- Monopolar cautery
- Chalazion clamp
- Chalazion scoop
- Dexamethasone 4 mg/ml injection
- Gauze
- Eye patches
- Westcott scissors and 0.5 mm forceps may be needed
- Pathology specimen pot may rarely be needed
Surgical Steps:
- Soak the conjunctival surface with topical xylocaine drops or gel
- Evert the eyelid
- Apply the Gate theory (tapping, massage, rubbing of hands, arms, legs, etc) to reduce the perception of discomfort during the injection of local anesthetic
- Infiltrate the lesion with local anesthetic
- Apply the chalazion clamp and evert the eyelid
- Incise vertically over the affected Meibomian gland
- Curette the contents with a chalazion scoop
- Apply pressure to the treated and surrounded glands (see video) to ensure any other affected glands are also drained
- If there is a bleed, simple local cautery may be applied although this is rarely needed
- Some people apply carbolic acid to the cavity: we have not used this in our patients
- The eyelid will ooze for a few minutes: simple pressure will resolve this
- Application of ointment and a monocular occlusive dressing may be used
- When a chalazion is pointing anteriorly or has burst through the anterior surface of the eyelid, it is reasonable to perform curettage via the anterior of the eyelid
- Any granulomatous tissue is removed with sharp dissection
- Patients (usually men) will sometimes feel faint at the end of the procedure. It is best to leave the head reclined until the patient is feeling well enough to stand

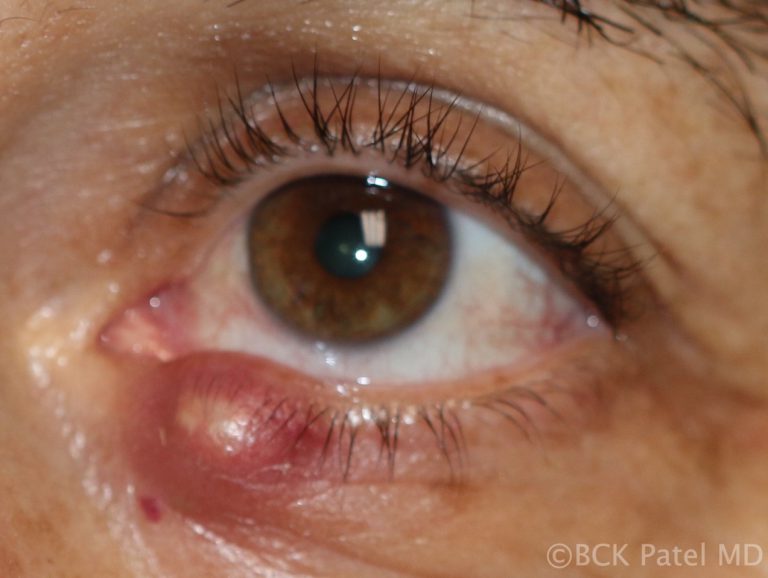
Chronic Chalazia
Chronic chalazia are chalazia that have been present for many weeks to months and are usually firm and painless. These are best treated with local anesthetic injection, incision and curettage, together with dexamethasone injection. We apply our two-finger firm pressure technique to break down any surrounding areas which may have chronic material in them. The patient should be warned that the bulk of the lesion will reduce in size over the subsequent few days but the final resolution can often take many weeks. Patience is key here…..

Giant Chalazion

These are large chronic chalazia and will often look like they are occupying the whole eyelid. They will frequently emanate from multiple Meibomian glands so it is important to drain all of them properly

Chalazia in Children


Children will often present with chalazia, often multiple and frequently recurrent. There is no known cause of this and most will settle with conservative management discussed above. Parents can get frustrated by the recurrent chalazia that some children get. We always reassure them that they eventually resolve and do not leave any underlying scarring of the eyelids. In some cases oral antibiotics like Azithromycin are indicated

Chalazion in patients with skin of color

Whereas the management of chalazia in patients who have skin of color is the same as in white Caucasians, care must be taken not to inject with steroids superficially as hypopigmentation may occur.
References
- Jordan GA, Beier K. Chalazion. StatPearls, Treasure Island (FL): StatPearls Publishing. Aug 2021.https://pubmed.ncbi.nlm.nih.gov/29763064/PMID:29763064
- WillmannD, Guier CP, Patel BCK,, Melanson SW. Stye. StatPearls, Treasure Island (FL): StatPearls Publishing. Aug 2021. https://pubmed.ncbi.nlm.nih.gov/29083787/ PMID:29083787
- Lindsley K, Nichols JJ, Dickersin K. Non-surgical interventions for acute internal hordeolum. Cochrane Database Syst Rev 2017 Jan 9;1(1):CD007742 PMID:28068454