
To read a blepharophimosis chapter by Prof BCK Patel MD, FRCS published in a textbook, please read below


What is blepharophimosis syndrome?
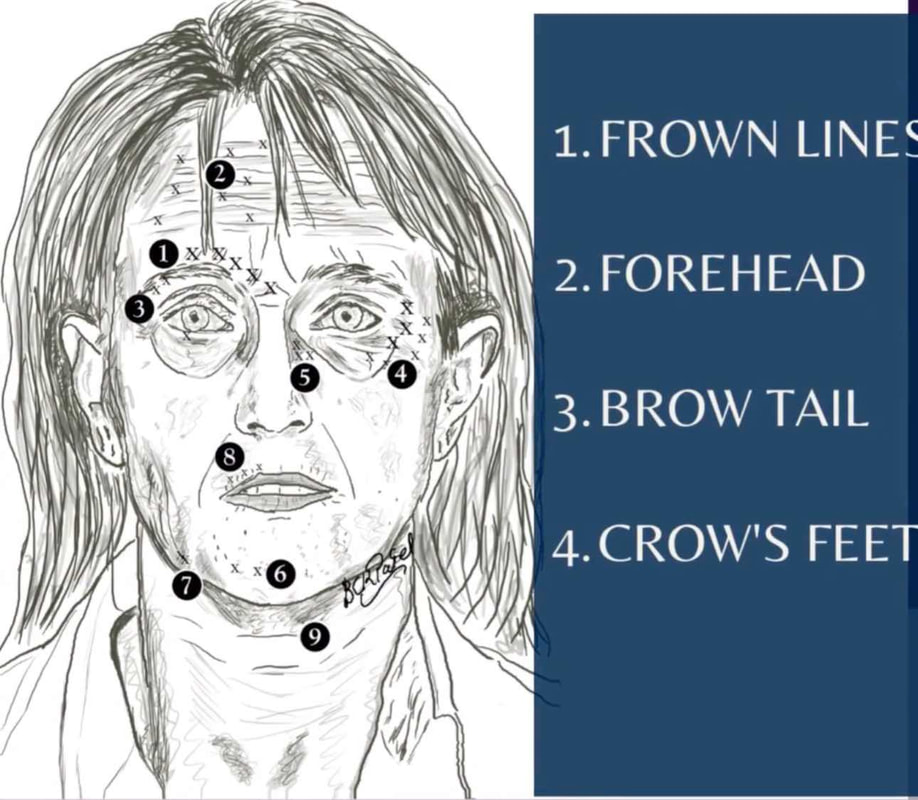
Blepharophimosis is from the Greek blepharon (eyelid), and phimosis (stricture).
Blepharophimosis Syndrome is also known as the Blepharophimosis, Ptosis, Epicanthus inversus Syndrome, usually abbreviated as "BPES"
Blepharophimosis Syndrome causes the palpebral aperture to be small both, horizontally and vertically. It may be associated with a variety of other condition.
Blepharophimosis Syndrome causes the palpebral aperture to be small both, horizontally and vertically. It may be associated with a variety of other condition.

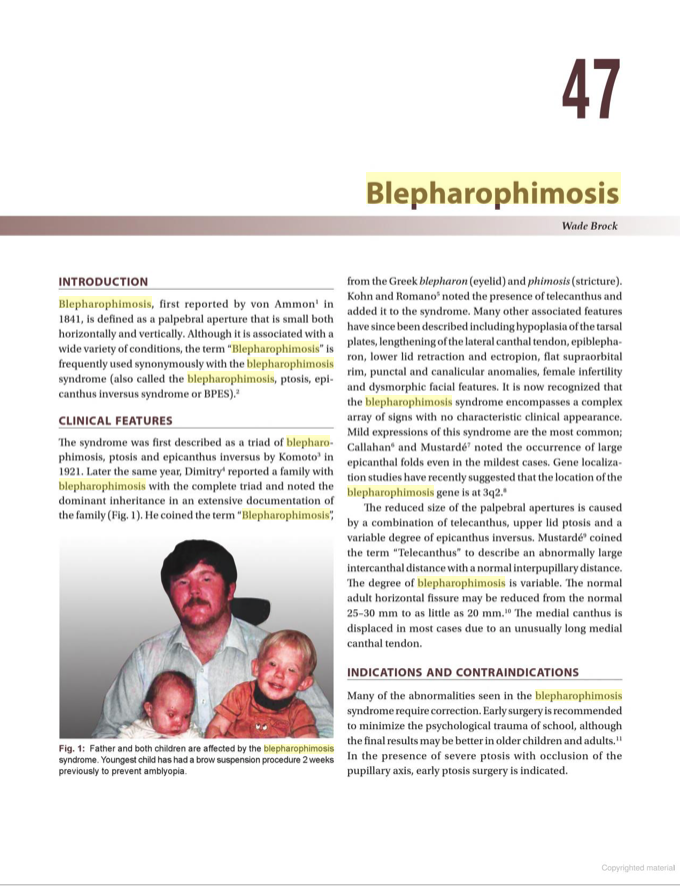
Autosomal Dominant Blepharophimosis Syndrome with blepharophimosis, ptosis and epicanthus inversus
blepharophimosis syndrome (BPES)
Blepharophimosis Syndrome is now known to have the following findings:
- Blepharophimosis
- Ptosis
- Epicanthus Inversus
- Telecanthus (added to the syndrome by Kohn and Romano): long medial canthus which reduces the horizontal fissure from the normal 25 - 30 mm to as little as 20 mm
- Hypoplasia of the tarsal plates
- Lengthening of the lateral canthal tendon
- Epiblepharon
- Lower eyelid retraction
- Eyelid ectropion
- Flat supraorbital rim
- Punctal anomalies
- Female infertility may occur
- Amblyopia may be found in more than 50% of patients
- Strabismus is found in 26.7%
- Gene localization studies indicate that the location of the blepharophimosis gene is at 3q2
“Fortunately, for us, Dr. Patel at Primary Children’s Hospital – Moran Eye Center, was equally comforting as he was qualified. He has phenomenal bedside manners, and is an extremely kind human being. Nothing about our experience with him made us feel like he was in a routine, or that he’d seen this a thousand times, he treated us as friends, and as if he was bearing this burden with us.”
Parents of child with Blepharophimosis Syndrome, USA
Parents of child with Blepharophimosis Syndrome, USA
|
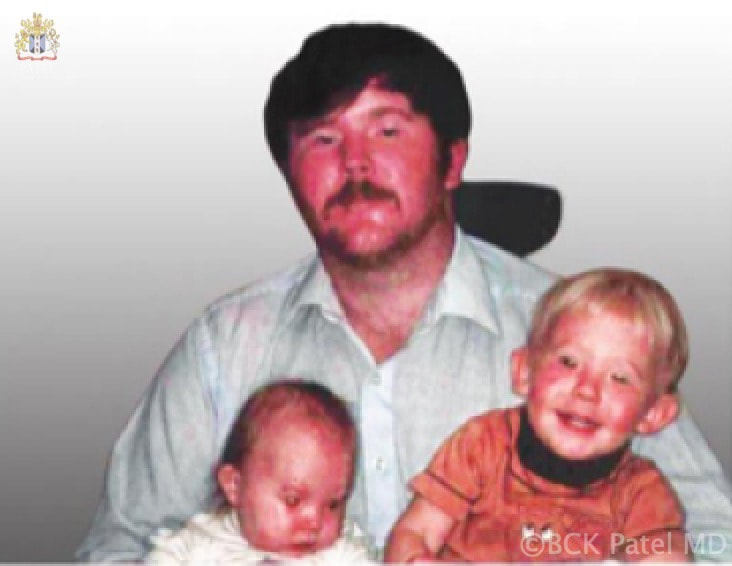
Autosomal Dominant Blepharophimosis Syndrome with dad and both children affected
management of Blepharophimosis syndromeMost children with the Blepharophimosis Syndrome will have a ptosis (droopy upper eyelids) with poor levator function. The following will be seen:
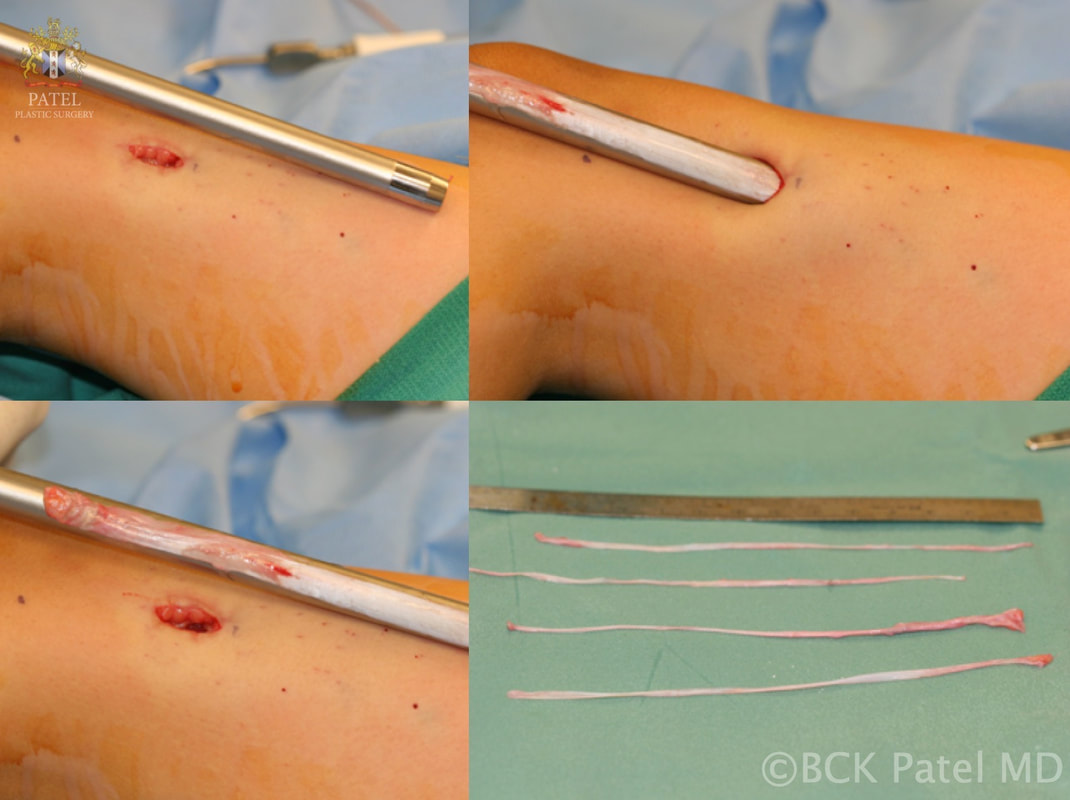
Once the child is older, and when the more permanent slings need to be performed, we use autogenous fascia lata to lift tye lids. |


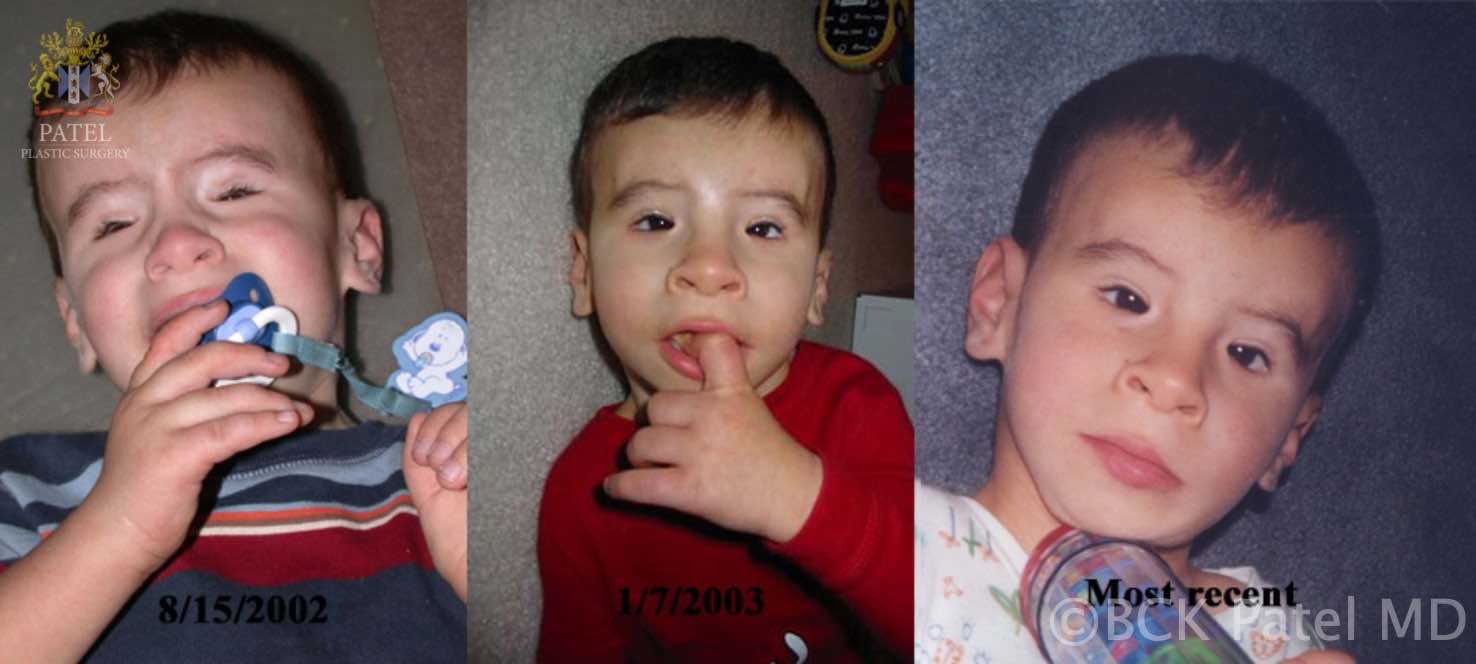
Blepharophimosis Syndrome with severe ptosis and phimosis and telecanthus. Photos after frontalis slings to allow visual development. The telecanthus repair will be performed when the child is older to give the best cosmetic results
"Why don't we have more doctors like this doctor? He really knows his stuff but he is also very patient and explains things clearly.
I had botched surgery and had too many operations (five). Every time someone would see me they would want to operate and I was always left worse off. I finally was very frustrated and did not want to come from Montana and drive 8 hours just to see yet another doctor but I am so glad I did. My eyes are so much more comfortable now after Dr. Patel's care and I even look better. He took his time analyzing all my procedures and planning things and I will always be grateful to him and to the University for having this great doctor.
W.E 53 Yrs Old with "trouble until I came here!"- Billings, MT
I had botched surgery and had too many operations (five). Every time someone would see me they would want to operate and I was always left worse off. I finally was very frustrated and did not want to come from Montana and drive 8 hours just to see yet another doctor but I am so glad I did. My eyes are so much more comfortable now after Dr. Patel's care and I even look better. He took his time analyzing all my procedures and planning things and I will always be grateful to him and to the University for having this great doctor.
W.E 53 Yrs Old with "trouble until I came here!"- Billings, MT
total management of blepharophimosis syndrome
The sequence of repair is to perform the droopy-eyelid surgery with frontalis slings as soon as possible, followed by repair of the telecanthus some years later once the nasal bridge has developed somewhat.
Over time, the slings will relax. In the beginning (immediately after surgery), it is understandable that parents will be surprised to see the eyelids wide open and even open when the child sleeps: this relaxes and, fortunately, does not seem to bother our children. However, we will give you simple instructions so that the corneas may be kept lubricated. This applies to all frontalis sling procedures, whether performed in children with the Blepharophimosis Syndrome or with severe congenital ptosis
Over time, the slings will relax. In the beginning (immediately after surgery), it is understandable that parents will be surprised to see the eyelids wide open and even open when the child sleeps: this relaxes and, fortunately, does not seem to bother our children. However, we will give you simple instructions so that the corneas may be kept lubricated. This applies to all frontalis sling procedures, whether performed in children with the Blepharophimosis Syndrome or with severe congenital ptosis

Blepharophimosis Syndrome with severe ptosis and phimosis and telecanthus. Photos after frontalis slings to allow visual development and repair of the telecanthus. The lower eyelid retraction and cheek ptosis have also been repaired
How is Congenital Ptosis with poor levator function repaired?
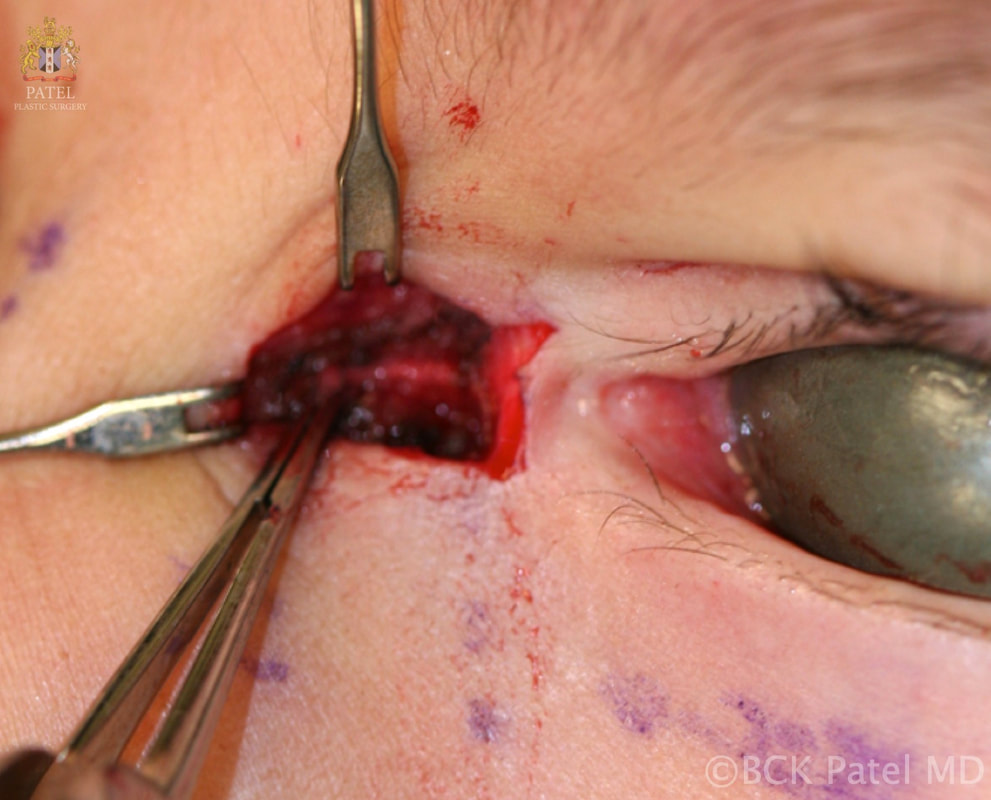
Dr. Patel uses the "micro-incision" approach to insertion of frontalis slings so the scarring is minimal. Indeed, most parents cannot see our scars after a few months (see photos above and below). Similarly, when repairing the telecanthus, the lateral canthal malposition and the cheek hypoplasia, cosmetic principles are applied to give gratifying results
Careful followup and repair of the different structures yields excellent results in the Blepharophimosis Syndrome. The old medial canthoplasties used to leave patients with extensive scars even though they corrected the telecanthus, so Dr. Patel uses the technique he designed and applying cosmetic principles to this surgery, excellent results are obtained
|
|
|
|
|
|
|
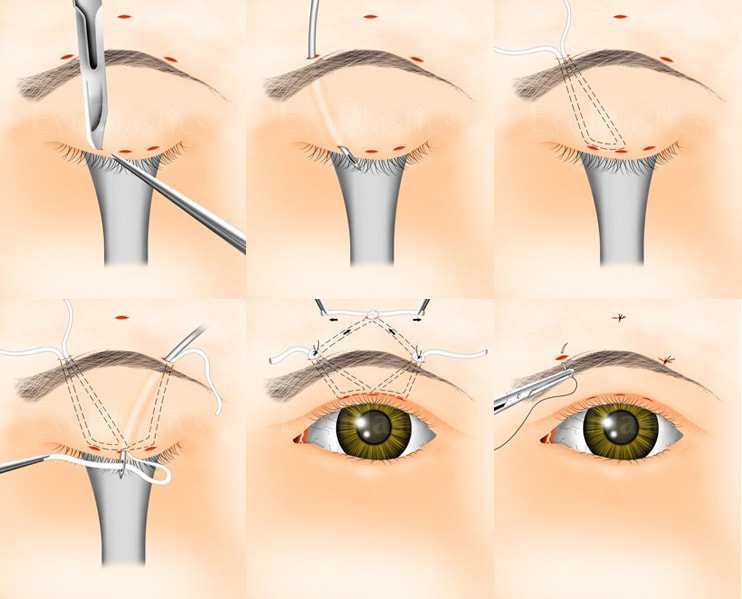
Frontalis SlingWhen the weakness is profound, with little or no function, “frontalis slings” are performed. Before a child is 4 or 5 years old, temporary materials are used to elevate the eyelids so that vision may develop more normally.
When the child is older, fascia lata is obtained from the leg to perform slings. The fascia lata slings last much longer as the material is autogenous. |
|

Accurate measurements and markings of palpebral fissures and telecanthus to design the repair of the canthal tendons after the fascia lata frontalis slings have been inserted

|
|




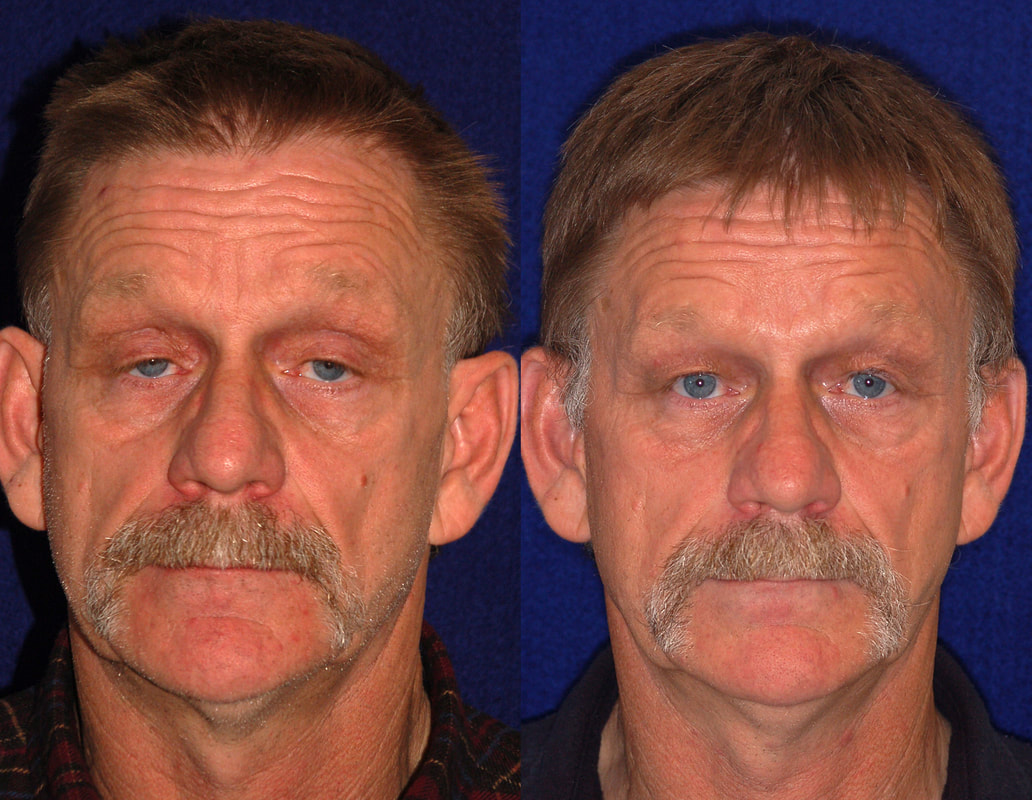
Before and After photographs after use of frontalis slings in children and adults

|

|



|


|
"I had a excellent eye lift done by Dr. Patel. He knows what he is doing and is very pleasant. Dr.Patel was easy to get an appointment and he works with you. The office staff was very pleasant and made you feel calm." D. Gull Highly recommended for eye lift surgery - Salt Lake City, UT
Will the frontalis sling ptosis surgery need to be repeated?
The initial frontalis slings use goretex or silicone material and last for a number of years. Once the child is five years or older and if the lids droop again, then fascia lata slings are performed. These last for many decades. Even when the child has essentially no levator function, we are able to design a very attractive upper eyelid and crease. Small asymmetries will remain as all this is "man-made"!
What care will I need to give my child after ptosis Surgery
Whether a direct levator advancement procedure is performed or a frontalis sling is performed, it is normal for the child to sleep with the eyelids somewhat open: this may be dramatic in the beginning but the degree of opening reduces over time. However, the lids may stay open to some degree for a long time or forever. This is normal and every child will experience this. After surgery, the following instructions should be followed: Incisions which are hidden in front of and behind the ear. Once healed, they are close to invisible.
- The incision sites will need the application of erythromycin eye ointment three times a day for about a week: this will be prescribed.
- It will be important to keep the incision sites clean: clean hands!
- Any oral antibiotics prescribed (especially important when frontalis slings are performed) must be administered.
- For the first few weeks, applying a small amount of eye lubricating ointment (Refresh pm ointment or any other eye lubricating ointment will do) whenever the child sleeps or takes a nap is important. After a few weeks, most children do not need continud application of ointment unless they are unwell or have a cold. We will guide you.
- Most children see so much better once the eyelid/eyelids have been lifted that you will notice them being much more physically active! This all to the good!
- If patching was prescribed by the paediatric ophthalmology team, please continue with the patching until you see the team again: they will reduce or stop the patching once appropriate.
- Most children can return to school within three or four days. There is very little pain after this surgery: children’s Tylenol is usually sufficient.
- We will monitor the eyelid height once every six to nine months; the paediatric ophthalmology team will assess visual development and examine you for any strabismus or need for patching as well.
What sort of scars will there be?
When a direct incision is made to lift the eyelid, the incision is hidden in where a natural crease would form. All children heal with a pink scar initialy, but this is almost invisible after a few months. After frontalis slings, the incisions become almost invisible within a few months as we make very small incisions using a technique that we developed at the University of Utah and have taught to surgeons from all over the world. We take pride in our “small-incision” frontalis slings with minimal scars, unlike the way the surgery is performed in many other centers. It is normal to feel small bumps under the skin after frontalis slings as the sling material is attached to the frontalis muscle:
however, these are rarely visible.
however, these are rarely visible.
"Dr.Patel such a wonderful person...trust worthy, making u feel like family, included his staff members. Made my worries go away with there caring ways. God bless them. He truly make a wonderful job...it seem like a miracle. Dr. Patel makes magic happen." -Vitals.com Visitor Review

Visit Patel Plastic Surgery on YouTube for more free tips!
Stay Connected With Us On Social Media
|
Find UsLocations:
Dr. BCK Patel MD, FRCS 1025E 3300S Salt Lake City, Utah 84106, USA (801) 413-3599 (phone/text) E: [email protected] bckpatel.info --------------------------------------- Dr. BCK Patel MD, FRCS 585 E Riverside Dr Suite 201 Saint George, UT 84790 (435) 215-0014 E: [email protected] Quick-Link |
Let Us answer your questions |