recurrence of pterygium
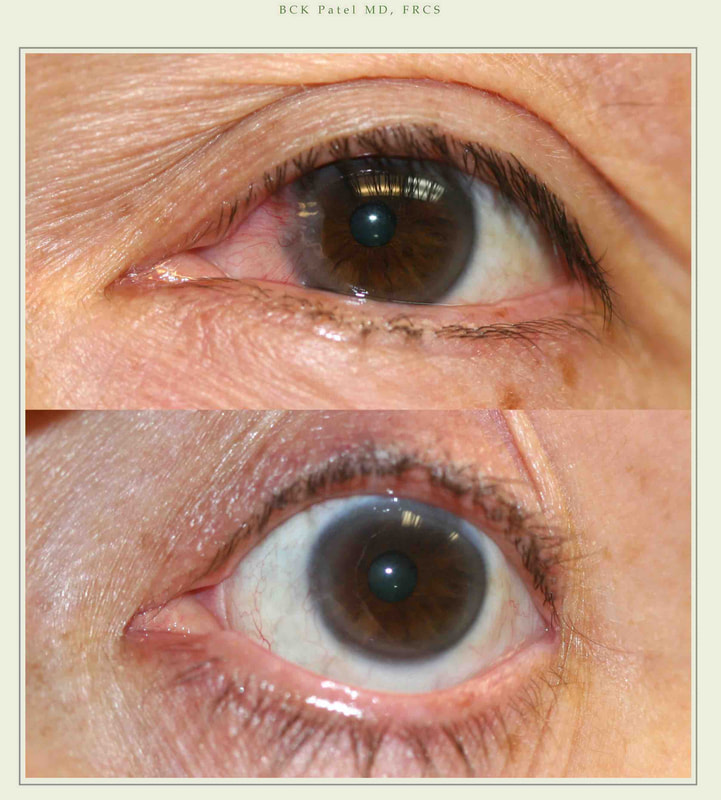
All operations have success and failure rates. Fortunately, with the modern techniques we use, recurrence of a pterygium is now rare. However, if one does not protect the eye from ultraviolet light, heat and dust and if artificial tears are not used as needed, there is a higher risk of recurrence of the pterygium. Some degree of redness of the graft and surrounding tissues will remain but this is not a recurrence.
Time off work
If your work involves heavy lifting or a lot of computer time, you would be wise to get a week off work.
Depending upon your specific requirements, we will be happy to give you a note for work.
What if i have had surgery somewhere else and i have a recurrence
Please bring photographs of your condition prior to surgery and your operation report when you come to see us. We will examine you and give you information on how matters can be improved.
Discomfort
Surprisingly, most patients find they get very little discomfort after this surgery. You may need the prescription pain medication for one or two days; thereafter, simple over-the-counter pain medication like Tylenol suffices.
How long does it take to get preauthorization from my insurance company?
Preauthorization may take four to six weeks from the time of submission of your information to the insurance company: we don’t have control over this, unfortunately.
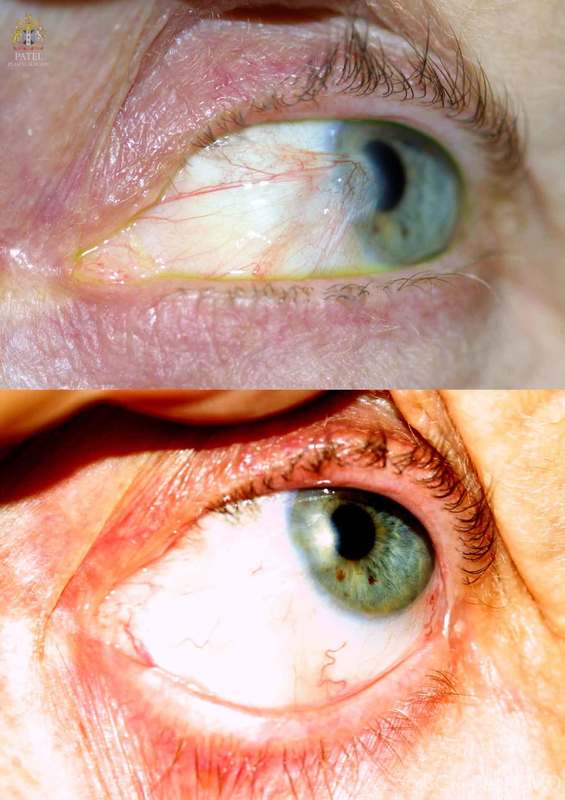
pingueculae
Often, patients will have a pterygium on one side which we will operate upon and either a small pterygium or a pingueculum on the other eye. All of these do not need surgery. If you begin to protect your eye from ultraviolet light and reduce dryness and direct heat injury to the eye (work, play, etc), you can slow down the growth of these pingueculae. If you do not have any symptoms and the growth is not distorting the cornea, there is no need to undergo surgery.
Do I Need This Surgery?
Only if the pterygium causes irritation, dryness, or problems with vision
We will review your history and examine you: this will allow us to guide you as to whether the surgery may or may not be necessary.
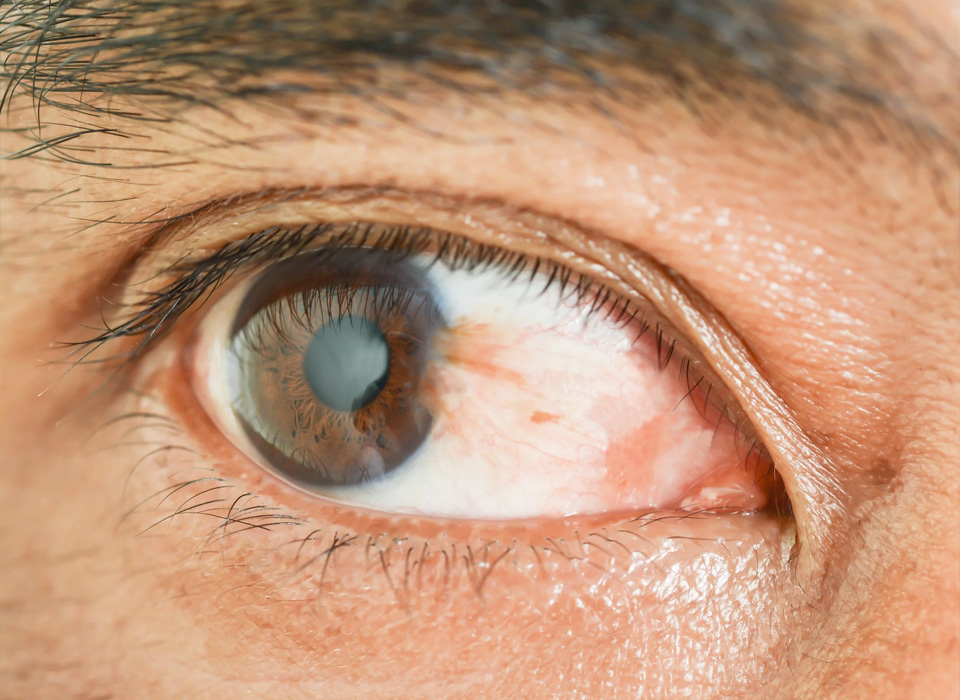
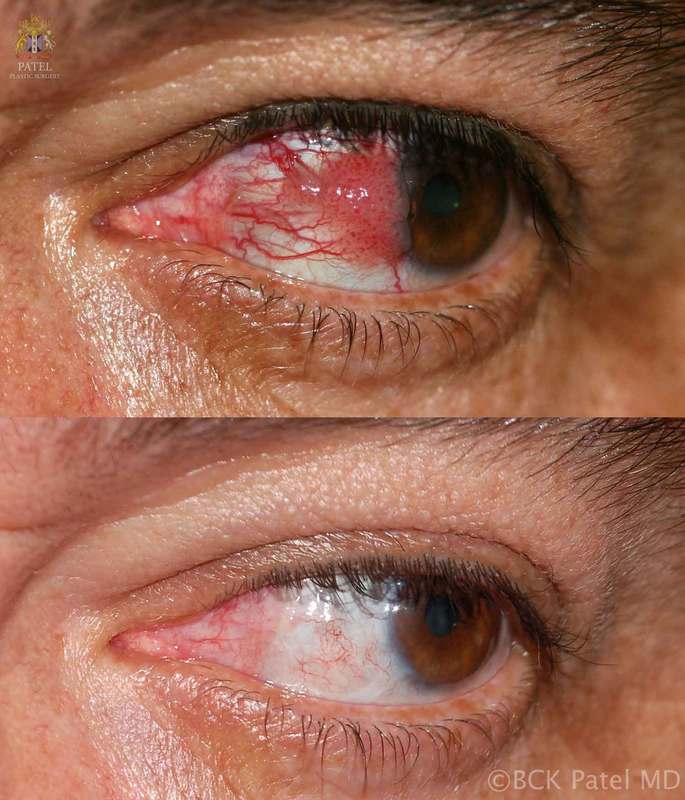
Persistent redness
This is seen, as has been discussed above, with the chronic sun damage we often see in sunny climes: therefore, you should expect some degree of redness with dilated vessels which are the result of such chronic injury. Some redness of the graft is also to be expected. The chronic use of vasoconstrictor drops is NOT recommended.
Will my pterygium surgery be covered by Insurance?
Most insurances cover the surgical operation when it is performed for the appropriate reasons. If your insurance requires the submission of your history, findings and photographs to get pre-approval, we will ensure we do this.