
To read a peer-reviewed medical article on ptosis in myasthenia gravis by Prof BCK Patel MD, FRCS & team, published in the British journal of ophthalmology, please read below


Important
Ptosis repair in myasthenia Gravis is NOT permanent as the disease involves variable but ongoing weakness of the muscle. Further surgery, sometimes with slings is always needed and this varies from person-to-person depending upon the change of the underlying muscle
What is myasthenia gravis?
myasthenia gravis is from the Greek myasthenia (muscle weakness), and the latin word gravis (serious).
Myasthenia Gravis (MG) is an autoimmune disease: postsynaptic acetylcholine receptors at the neuromuscular junction of skeletal muscles are targeted: the result is muscle weakness which shows fatigability. Blocking of neuromuscular transmission occurs, causing the muscle weakness.

Myasthenia gravis with severe asymmetric ptosis and lower lid retraction with brow overaction
|
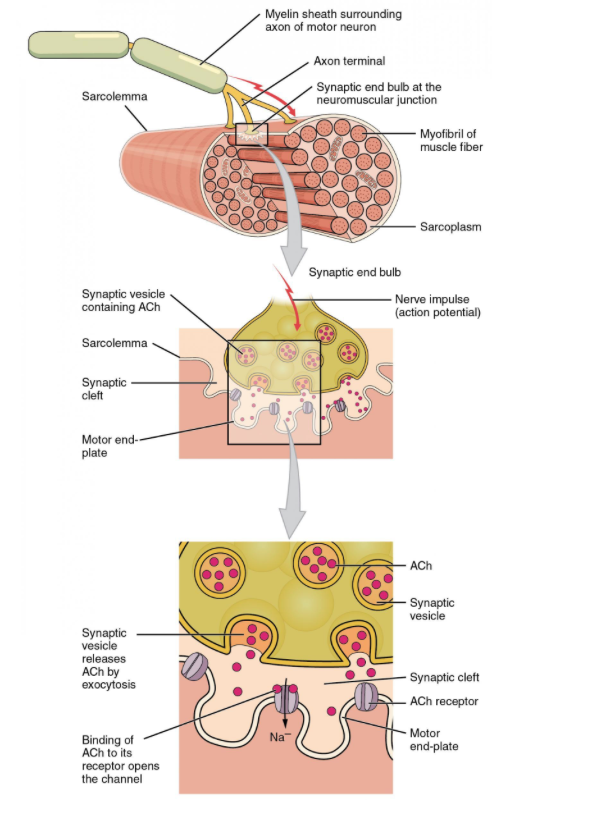
Motor endplate innervation
|
how does myasthenia gravis present?
The disease essentially presents with muscle weakness which worsens with muscle use (the muscles fatigue). The symptoms are generally worse later in the day for that reason.
- At initial presentation, more than 50% of patients will have ocular symptosms (droopy upper lids - ptosis, or double vision because of the involvement of the extraocular muscles
- Nearly 90% of patients with myasthenia gravis have eventual involvement of the ocular muscles
- Approximately 50% of patients who are seen with initial ocular weakness will develop generalized weakness within 3 years of initial presentation
- About 25% of patients will only have ocular findings and no generalized muscle weakness. There is a thought that over time, this number decreases
- About 5% of patients present initially with limb weakness (proximal is more severe than distal)
- It is common to undergo exacerbations so that the weakness my vary from ile to severe over time
- Difficulty in swallowing, slurred speech, chewing difficulty, facial weakness
- Muscle weakness is worsened by activity and improves with rest. Hence the droopy upper lids are better in the morning or after sleep
“Fortunately, for us, Dr. Patel at Primary Children’s Hospital – Moran Eye Center, was equally comforting as he was qualified. He has phenomenal bedside manners, and is an extremely kind human being. Nothing about our experience with him made us feel like he was in a routine, or that he’d seen this a thousand times, he treated us as friends, and as if he was bearing this burden with us.”
Parents of child with Blepharophimosis Syndrome, USA
Parents of child with Blepharophimosis Syndrome, USA
|

Marked ptosis in myasthenia gravis patient with worsening of the droop towards the end of the day when the patient was examined
how is myasthenia gravis diagnosed?
|
clinical assessment of myasthenia gravis
- The ptosis can be shown to worsen if the patient is asked to sustain an up-gaze for two to three minutes
- The Herrings Law is "more significantly positive" in patients with MG
- "The Peek Sign": sustained squeezing of the eyelids (orbicularis oculi muscle) will show weakening and the sclera will become visible with the eyelids partially open
- By sustaining lateral gaze, diplopia may be elicited
- Arm weakness may be apparent by sustained abduction of the arms (arms held out away from the body)
- Patients with involvement of the nasal and lingual muscles will show fatiging when counting aloud from 1 to 50
- Patient unable to keep the leg raised whilst lying down
- Repeated standing from a chair will show fatiguing
- Hyperthyroidism is seen in up to 15% of patients with MG (more commonly seen with ocular MG) and treatment of one does not improve the other disease
"Why don't we have more doctors like this doctor? He really knows his stuff but he is also very patient and explains things clearly.
I had botched surgery and had too many operations (five). Every time someone would see me they would want to operate and I was always left worse off. I finally was very frustrated and did not want to come from Montana and drive 8 hours just to see yet another doctor but I am so glad I did. My eyes are so much more comfortable now after Dr. Patel's care and I even look better. He took his time analyzing all my procedures and planning things and I will always be grateful to him and to the University for having this great doctor.
W.E 53 Yrs Old with "trouble until I came here!"- Billings, MT
I had botched surgery and had too many operations (five). Every time someone would see me they would want to operate and I was always left worse off. I finally was very frustrated and did not want to come from Montana and drive 8 hours just to see yet another doctor but I am so glad I did. My eyes are so much more comfortable now after Dr. Patel's care and I even look better. He took his time analyzing all my procedures and planning things and I will always be grateful to him and to the University for having this great doctor.
W.E 53 Yrs Old with "trouble until I came here!"- Billings, MT
management of myasthenia gravis
There has been impressive progress in the management of myasthenia gravis as we now understand that therapy may be focused based upon a number of factors, including the different antibodies involved, the differences in clinical presentation, the age of onset, presence or absence of thymic involvement, and the weakness distribution.
A brief summary of management is as follows (careful assessment and treatment are by neurologists or neuromuscular specialists):
A brief summary of management is as follows (careful assessment and treatment are by neurologists or neuromuscular specialists):
- Anticholinesterase inhibitors with pyridostigmine for maintenance treatment (neostigmine is used when pyridostigmine is not available)
- Intravenous immune globulin
- Prednisone as an immunosuppressive agent for long-term maintenance therapy
- Azathioprine may be used as a steroid-sparing agent
- Mycophenolate mofetil has been found to also be steroid-sparing and less toxic than azathioprine
- Cyclosporine. Methotrexate and Tacrolimus are other steroid-sparing agents
- Rituximab has been found to be effective in refractory MG
- Cyclophosphamide is used in severe or refractory MG
- There are a number of newer monoclonal antibodies that are being tested and hold much promis
- It has been shown that a thymectomy improves MG and may reduce or eliminate the need for systemic medication. All patients with myasthenia gravis are worked up for involvement of the thymus and considered for a thymectomy

Asymmetric ptosis in myasthenia gravis is common and may require asymmetric surgery. It should be remembered that the lid position will vary through the day and will eventually need further surgery
what are the ocular findings in myasthenia gravis?
As mentioned, ptosis and double vision are common and over time, more than 90% of patients with MG will demonstrate ocular findings. The ptosis is minimal early in the morning and worsens through the day. The ptosis may be asymmetric.
Double vision may be intermittent of constant. Initially, patients may present with just blurred vision. Pupil function in MG is always normal.
Double vision may be intermittent of constant. Initially, patients may present with just blurred vision. Pupil function in MG is always normal.

Advanced myasthenia gravis with marked facial weakness: frontalis muscle weakness (brow ptosis), upper lid ptosis, lower lid laxity and ectropion and cheek ptosis with loss of facial expression
Assessment of Ptosis in myasthenia gravisPtosis repair requires careful assessment of patients with myasthenia gravis because of a number of other factors that may affect the choice and procedure for ptosis correction. Specifically,

Ptosis is almost always asymmetric in myasthenia gravis and varies greatly from morn to dusk! Correction is an art, not a science and the lower eyelids and Bell's phenomenon need to be carefully examined
|

Repair of ptosis with levator advancement in myasthenia gravis. At the end of the day, the upper lids are droopy but much improved. Over time, the lids will need further surgery, sometimes slings
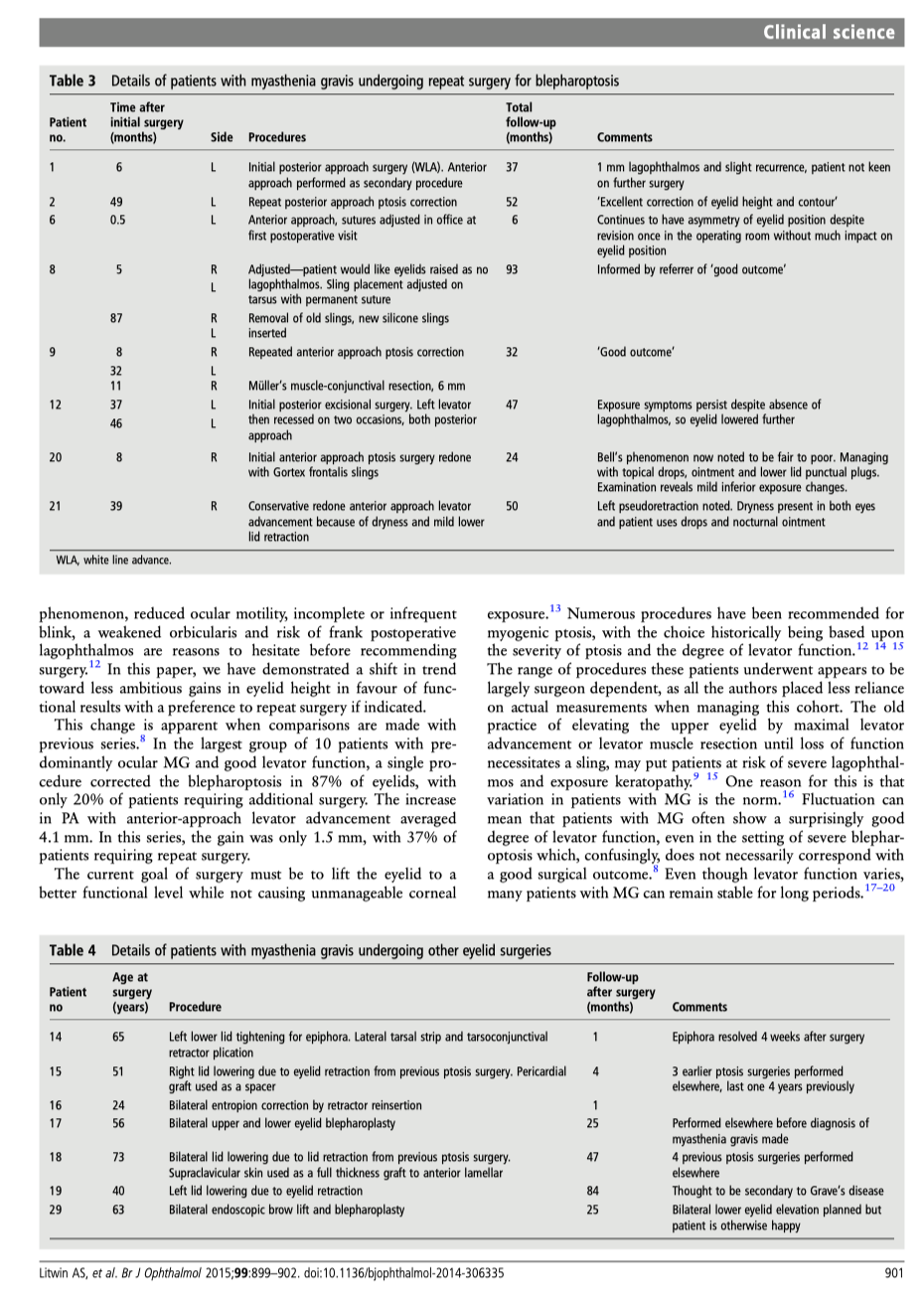
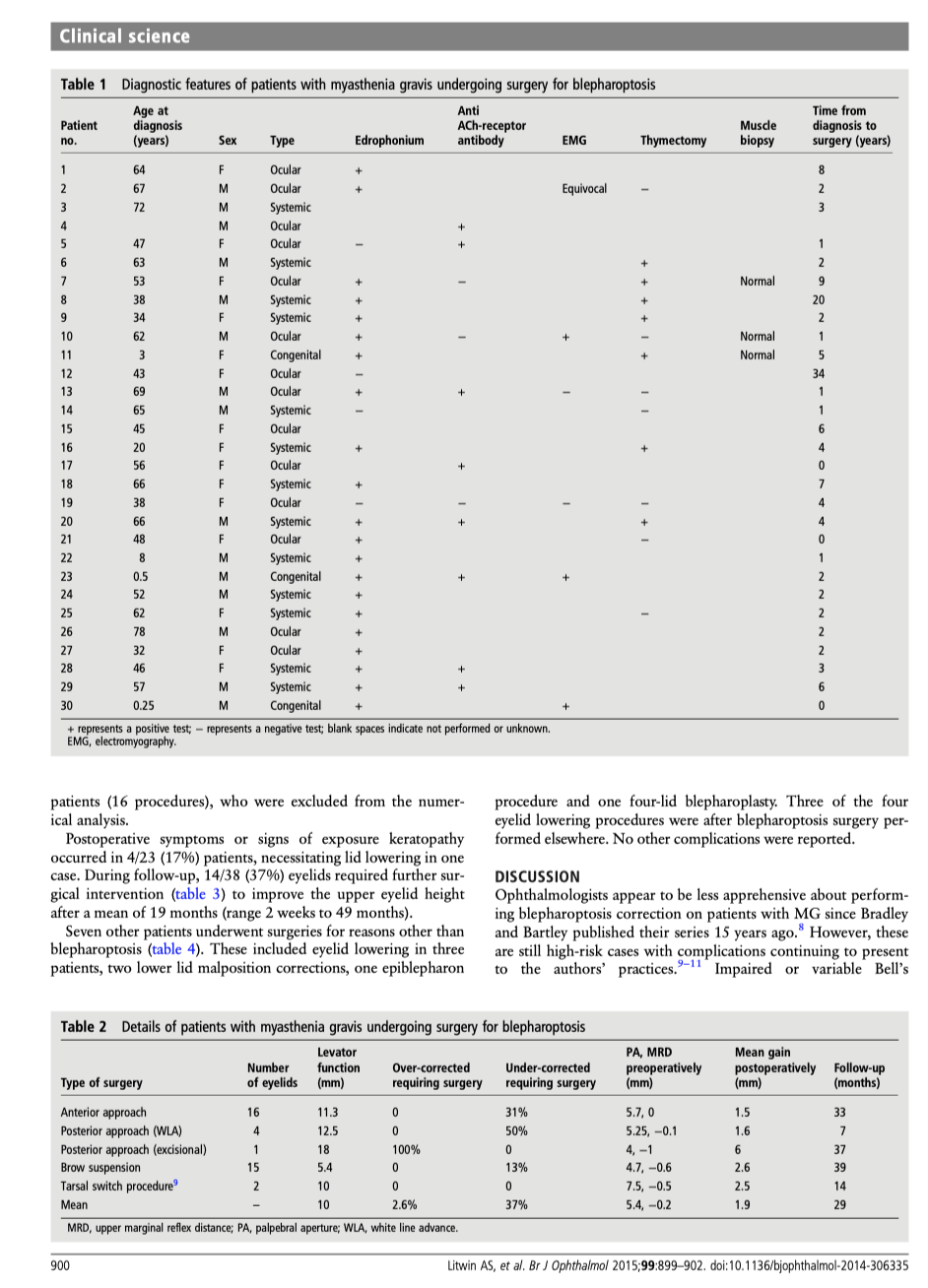
Ptosis repair in myasthenia gravisIn a comprehensive review of patients we repaired and followed, we have shown the following:
|

Brow ptosis, ptosis and lower lid laxity, retraction and cheek ptosis in myasthenia gravis: all the related findings need to be examined and assessed so as to choose the correct procedures in Myasthenia Gravis
"I had a excellent eye lift done by Dr. Patel. He knows what he is doing and is very pleasant. Dr.Patel was easy to get an appointment and he works with you. The office staff was very pleasant and made you feel calm." D. Gull Highly recommended for eye lift surgery - Salt Lake City, UT
Brow ptosis in myasthenia gravis
Because of facial muscle weakness, some patients will develop severe forehead (frontalis muscle weakness) and brow droop with secondary dermatochalasis and difficulty with vision.
Such patients need elevation of the brows.
Such patients need elevation of the brows.
- So-called internal browlifts will not work and are not recommended
- A direct brow lift may be performed
- We designed and presented a form of a mid-forehead brow lift which allows us to improve the forehead and brows with excellent results functionally and cosmetically
- Endoscopic brow lifts which we use in cosmetic brow elevation will not work long-term in patients with MG
- String-browlifts, suture-browlifts and other minimally invasive techniques will not work in patinets with MG

Correction of the frontalis muscle and brow ptosis as well as the lower lid laxity but conservative upper lid surgery allows the patient to see but to also close the eyelids and thereby protect the corneas
myasthenia gravis in children
Myasthenia gravis may be seen in newborns when the mother is affected by MG. The MG here is transient. Only about 20% of infants born to mothers with MG will develop neonatal MG.
If MG persists, then treatment of the droopy upper lids is needed.
If MG persists, then treatment of the droopy upper lids is needed.

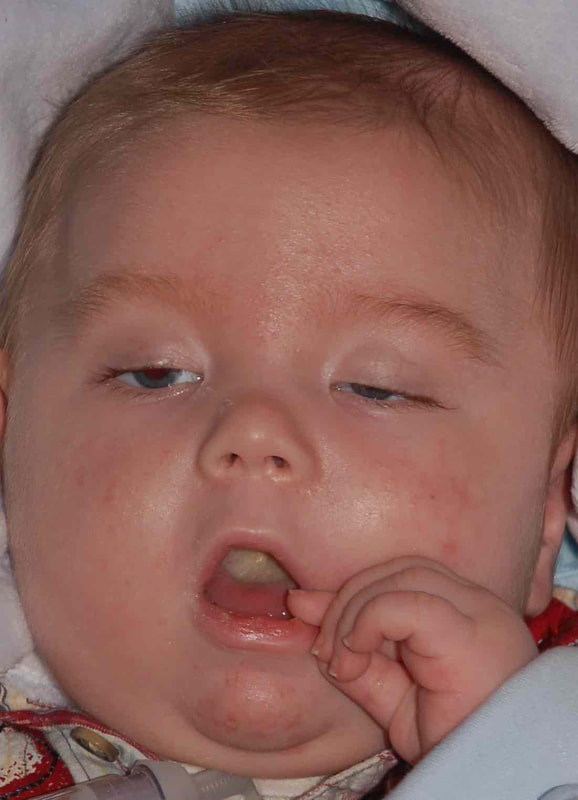
Severe ptosis in a child with myasthenia gravis treated with frontalis slings which allow the child to open the eyelids and also close them well enough to protect the corneas
care of upper eyelids after ptosis Surgery
Some degree of difficulty closing the eyelids for the first few days is normal and to be expected.
After surgery, the following instructions should be followed:
After surgery, the following instructions should be followed:
- The incision sites will need the application of erythromycin eye ointment three times a day for about a week: this will be prescribed.
- It will be important to keep the incision sites clean: clean hands!
- Any oral antibiotics prescribed (especially important when frontalis slings are performed) must be administered.
- For the first few weeks, applying a small amount of eye lubricating ointment (Refresh pm ointment or any other eye lubricating ointment will do) whenever one naps or sleeps at night. After a few weeks, most people do not need continued application of ointment unless one is unwell (colds, illness, etc)
- The sutures dissolve over two weeks.
- During the day, lubrication with artificial tears may be needed for the first few weeks.
What sort of scars will there be?
When a direct incision is made to lift the eyelid, the incision is hidden in where a natural crease would form. Scars may have a few bumps (because of the deep sutures), but these disappear over time.
After frontalis slings, the incisions become almost invisible within a few months as we make very small incisions using a technique that we developed at the University of Utah and have taught to surgeons from all over the world. We take pride in our “small-incision” frontalis slings with minimal scars, unlike the way the surgery is performed in many other centers. It is normal to feel small bumps under the skin after frontalis slings as the sling material is attached to the frontalis muscle: however, these are rarely visible.
After frontalis slings, the incisions become almost invisible within a few months as we make very small incisions using a technique that we developed at the University of Utah and have taught to surgeons from all over the world. We take pride in our “small-incision” frontalis slings with minimal scars, unlike the way the surgery is performed in many other centers. It is normal to feel small bumps under the skin after frontalis slings as the sling material is attached to the frontalis muscle: however, these are rarely visible.
"Dr.Patel such a wonderful person...trust worthy, making u feel like family, included his staff members. Made my worries go away with there caring ways. God bless them. He truly make a wonderful job...it seem like a miracle. Dr. Patel makes magic happen." -Vitals.com Visitor Review

Visit Patel Plastic Surgery on YouTube for more free tips!
Stay Connected With Us On Social Media
|
Find UsLocations:
Dr. BCK Patel MD, FRCS 1025E 3300S Salt Lake City, Utah 84106, USA (801) 413-3599 (phone/text) E: [email protected] bckpatel.info --------------------------------------- Dr. BCK Patel MD, FRCS 585 E Riverside Dr Suite 201 Saint George, UT 84790 (435) 215-0014 E: [email protected] Quick-Link |
Let Us answer your questions |