
Graves' disease involves an overactive thyroid gland and results in an overproduction of thyroid hormones, or hyperthyroidism.
Graves' disease is an autoimmune condition. This meaning that the body's immune system mistakes healthy cells for foreign invaders and attacks them. It is the most common autoimmune disorder in the United States.
A number of conditions can cause hyperthyroidism, but Graves' disease is the most common, affecting around 1 in 200 people. It most often affects women under the age of 40, but it is also found in men.
Graves' disease was originally known as "exophthalmic goiter" but is now named after Sir Robert Graves (1796 - 1853), an Irish doctor who first described the condition in 1835. The name has been used wrongly as "Grave's disease" or "Graves disease". As it is named after Sir Robert Graves, the correct name is "Graves' Disease". If you are interested in the history of the man and the disease, you can read about it at our European Thyroid Association HERE.
Graves' disease is an autoimmune condition. This meaning that the body's immune system mistakes healthy cells for foreign invaders and attacks them. It is the most common autoimmune disorder in the United States.
A number of conditions can cause hyperthyroidism, but Graves' disease is the most common, affecting around 1 in 200 people. It most often affects women under the age of 40, but it is also found in men.
Graves' disease was originally known as "exophthalmic goiter" but is now named after Sir Robert Graves (1796 - 1853), an Irish doctor who first described the condition in 1835. The name has been used wrongly as "Grave's disease" or "Graves disease". As it is named after Sir Robert Graves, the correct name is "Graves' Disease". If you are interested in the history of the man and the disease, you can read about it at our European Thyroid Association HERE.
- Graves' disease is the most common cause of hyperthyroidism.
- It is the most common type of autoimmune disease in the United States.
- Graves' disease affects an estimated 2-3 percent of the world's population.
"Well, the last time I had a picture taken I could hardly see my eyes because of the weight of heavy eyelid. Then I paid attention to how I was actually using my eyes and I really noticed when I was looking at anything especially the computer I was straining my forehead to see better. Since I have had it done I no longer have to lift the forehead and tilt my head to see. It is amazing! I love..." D. Rock 63 Yrs Old with Fat Droopy Eyes - Salt Lake City, UT
Graves' eye disease (thyroid orbitopathy)
Due to the increased pressure on the optic nerves, untreated Graves' ophthalmology can lead to double vision and possibly partial blindness.
|
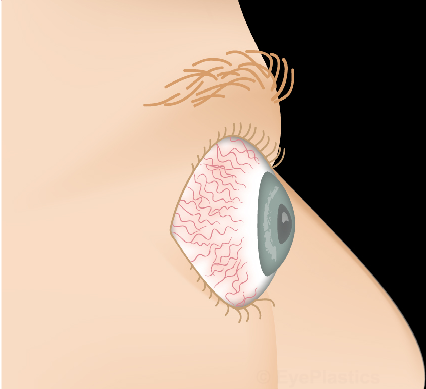
One feature of Graves' disease that is different from other types of hyperthyroidism, is its effects on the eyes. Graves' disease is the only type of hyperthyroidism that is associated with swelling and inflammation of the eye tissue.
Graves' eye disease, also known as thyroid ophthalmopathy (exophthalmos), affects around half of people with Graves' disease. The eyes can become:
|
It is still unclear why Graves' disease affects the eyes in this way. The severity of the condition does not correlate with the severity of eye symptoms; it can occur before the condition begins, or even without Graves' disease.
Thyroid Eye Disease
Thyroid eye disease may be seen with an overactive thyroid, a normal thyroid or an underacting thyroid. The eye disease has two phases: active and stable. The active phase usually lasts between six months and two years and is marked by inflammation. During this phase, medical treatment is administered to improve the eye symptoms.
During the second phase, the inflammation subsides (often called “burns out”). In this phase, there is decreased inflammation and more of a chronic change seen in the orbits and the eyelids. This has sometimes been called the “fibrotic phase”.
During the second phase, the inflammation subsides (often called “burns out”). In this phase, there is decreased inflammation and more of a chronic change seen in the orbits and the eyelids. This has sometimes been called the “fibrotic phase”.
Thyroid Eye Disease Treatment- Active INFLAMMATORY phase

Mild to moderate congestion with red, angry eyes, dilated episcleral and conjunctival vessels, injection over medial rectus insertion, mild conjunctivochalasis
|

Severe congestion with proptosis, marked injection, exposure, conjunctivochalasis, chemosis, corneal exposure and ulceration
|
controlling your hyperthyroidism
Thyroid eye disease (Graves' disease) only appears in 5 - 10% of people who develop hyperthyroidism. Sometimes it is seen with hypothyroidism and at other times where the thyroid levels are normal. Your thyroid status is assessed by your endocrinologist by not only looking at your thyroid levels, but also levels of antibodies. Some patients will have normal thyroid hormone levels but abnormal antibody levels: this is indicative of underlying thyroid abnormality.
Your endocrinologist will decide the best way to control your hyperthyroid status: some will start you on a medication like Methimazole. Other treatments include surgical thyroidectomy and another one is radioactive iodine treatment to "kill" the thyroid tissue. There are different approaches to the hyperthyroid status: you are best following your endocrinologist's advice. One treatment is not necessarily better than any of the other two.
Your endocrinologist will decide the best way to control your hyperthyroid status: some will start you on a medication like Methimazole. Other treatments include surgical thyroidectomy and another one is radioactive iodine treatment to "kill" the thyroid tissue. There are different approaches to the hyperthyroid status: you are best following your endocrinologist's advice. One treatment is not necessarily better than any of the other two.
Will removal of my thryoid or treatment with radioactive iodine affect my orbital disease ?
If you undergo a surgical thyroidectomy, the endocrinologist or surgeon will put you on a short course of oral prednisone. This is done as there were some reports that suggested that the orbital inflammation MAY be affected by the surgery: this is certainly not proven, but the use of the oral steroids after the thyroidectomy is a very reasonable treatment.
After your radioactive iodine treatment, should they decide to go that route, most patients are not put on oral steroids. However, those with inflammatory and active thyroid orbitopathy may need steroids: we would guide you with that.
Generally, it is important to remember that controlling the thyroid levels will not cure your thyroid orbitopathy. Also, some people assume that the antibodies will be under control once the hyperthyroidism is controlled and the thyroid orbitopathy will therefore be better. That is not the case. HOWEVER, it is important to get your thyroid status stabilized. Once they have it under control, you may be put on a thyroid medication supplement. Over time, thyroid orbitopathy "burns out" but the proptosis (bulging) may or may not change. The inflammation does reduce over time, so that discomfort, pain, etc improve. This, on average, happens over about 18 months after the start of the disease but the period is variable.
Links to Sites for More Information & Support Groups:
The American Thyroid Association has useful information on these subjects and you can read about it HERE.
The British Thyroid Foundation is one that I have supported and is one of the most informative sites out there. You can access it HERE.
The Graves' Disease and Thyroid Foundation has a useful forum section where information is shared You can access it HERE.
There are numerous other support groups around the world with excellent information. If you find one that is especially useful, please be so kind as to share it with me so that I can put it on this website for all my patients. We are always looking for ways to help and support patients with thyroid orbitopathy.
After your radioactive iodine treatment, should they decide to go that route, most patients are not put on oral steroids. However, those with inflammatory and active thyroid orbitopathy may need steroids: we would guide you with that.
Generally, it is important to remember that controlling the thyroid levels will not cure your thyroid orbitopathy. Also, some people assume that the antibodies will be under control once the hyperthyroidism is controlled and the thyroid orbitopathy will therefore be better. That is not the case. HOWEVER, it is important to get your thyroid status stabilized. Once they have it under control, you may be put on a thyroid medication supplement. Over time, thyroid orbitopathy "burns out" but the proptosis (bulging) may or may not change. The inflammation does reduce over time, so that discomfort, pain, etc improve. This, on average, happens over about 18 months after the start of the disease but the period is variable.
Links to Sites for More Information & Support Groups:
The American Thyroid Association has useful information on these subjects and you can read about it HERE.
The British Thyroid Foundation is one that I have supported and is one of the most informative sites out there. You can access it HERE.
The Graves' Disease and Thyroid Foundation has a useful forum section where information is shared You can access it HERE.
There are numerous other support groups around the world with excellent information. If you find one that is especially useful, please be so kind as to share it with me so that I can put it on this website for all my patients. We are always looking for ways to help and support patients with thyroid orbitopathy.
You should know
Burning eyesIt is important to restore lubrication during the active phase. The surface of the eye dries out because the eyelids are tight and do not blink properly. Inflammation may cause the tear glands to produce fewer tears. The degree of discomfort, especially in drier parts of the world (like Salt Lake City and Park City!). Liquid teardrops (or artificial tears) offer significant relief. Tips on using liquid teardrops:
Other tips:
|
Dry eyesWhen your eyes dry out, a reflex occurs, producing massive amounts of tears that flood the eye’s drainage system. The same reflex is observed when you begin to cry after smelling an onion. Unfortunately, your tears provide only short-term relief. As a rule of thumb, if your eyes produce excessive tears, they are probably dry. In dry eye, the outer covering of the eye is sometimes damaged and may be covered with small blisters.
Treatments include:
SteroidsAnti-inflammatory medications—chiefly steroids — are available for advanced causes of the disease. To avoid side effects associated with long-term use, steroids are given at higher doses for a month or so and then tapered off.
With careful monitoring, a second course of steroids can be prescribed for prolonged periods of inflammation. Also, steroids can be injected into the orbit during an office visit. These injections minimize side effects and cause minimal discomfort. In the early inflammatory phase, we usually put our patients on Diclofenac 25 mg per day and Acular drops twice a day: this combination is useful in reducing the degree of inflammation in the orbit and on the eyes without the use of oral steroids. Oral steroids, however, are needed in the more inflamed orbits and eyes. |
reducing the appearance of swellingUnfortunately, a great deal of swelling accompanies thyroid eye disease. You may notice bags under the eyes, increased bulging of the eyes, and swelling of the tissue coating the eyes. Anything that increases the fluid in the body can add to the swelling. Some solutions:
|
management of poor eyelid closureIf your eyes remain open during sleep (called lagophthalmos), you may experience severe drying that can damage the cornea. In some cases, the cornea may become ulcerated, resulting in loss of vision. One of the best ways to protect your eyes during the night is to make a Saran wrap dressing that serves as a moisture chamber.
|
Thyroid Eye Disease Treatment –
Stable Phase, after inflammation has subsided

Post-inflammatory phase with eyelid retraction and proptosis but no active inflammatory signs
Surgical Options
The combination of changes in thyroid orbitopathy that may need to be addressed include the following:
Dr. Patel has designed an approach which is termed “Cosmetic orbital decompression”, using minimally invasive techniques (as far as the patient and onlookers can see!), but with an advanced knowledge of the bony, muscular, fatty and soft tissue changes in this disease. Although traditionally, surgical approaches to the patient with thyroid orbitopathy was staged with bony orbital decompression followed by muscle surgery followed by eyelid surgery followed by any cosmetic surgery needed, Dr. Patel’s approach tries to reduce the number of different operations needed to improve the function and appearance of the eyes, orbits and eyelids.
- Proptosis (bulging of the eyeballs)
- Upper and lower eyelid retraction
- Lagophthalmos (inability to close eyelids adequately)
- Double vision
- Compression of the optic nerve with decrease in vision
- Pain
Dr. Patel has designed an approach which is termed “Cosmetic orbital decompression”, using minimally invasive techniques (as far as the patient and onlookers can see!), but with an advanced knowledge of the bony, muscular, fatty and soft tissue changes in this disease. Although traditionally, surgical approaches to the patient with thyroid orbitopathy was staged with bony orbital decompression followed by muscle surgery followed by eyelid surgery followed by any cosmetic surgery needed, Dr. Patel’s approach tries to reduce the number of different operations needed to improve the function and appearance of the eyes, orbits and eyelids.
First Stage- minimally invasive cosmetic orbital decompression surgery
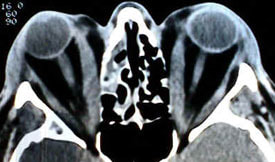
CT scans show type III orbitopathy with enlarged muscles but also increase in orbital fat. An accurate assessment of the type of orbitopathy and changes allows us to plan your surgery properly
|
After your clinical examination and review of the relevant orbital CT scans, Dr. Patel will be able to decide the best combination of procedures to give you the best result. We generally operate on one orbit, followed byt the other orbit about four weeks later to allow you to at least be functional with one eye. Our patients find this interval most useful.
During the orbital decompression surgery, a combination of bone removal and fat removal is performed, together with repositioning of the upper and lower eyelids, elevation of the cheek tissues, sometimes with a cheek onlay implant to give volume back to the midface. |
During the orbital decompression surgery, a combination of bone removal and fat removal is performed, together with repositioning of the upper and lower eyelids, elevation of the cheek tissues, sometimes with a cheek onlay implant to give volume back to the midface. The aim is to reduce the proptosis (bulging), as well as the eyelid procedures. If you have double vision, it will change for the better or worse temporarily. Generally, orbital surgery is not undertaken to improve double vision but to improve the bulging of the eye and the protection of the cornea. Once both orbits have recovered from the surgery, strabismus surgery (for ouble vision) may be performed.
- Reduce exposure of the surface of the eye
- Improve the eyelid’s ability to close over the eye
- Improve the bulging appearance
- Relieve pressure-pain

Proptosis, upper and lower eyelid retraction
|

after cosmetic orbital decompression and upper and lower eyelid repositioning
|

often, orbitopathy can be asymmetric. Here a right orbital decompression and bilateral eyelid repositioning allows a more symmetric appearance to be achieved.
|
Compression of the optic nerve with loss of vision
When there is compression of the optic nerve, you will first be treated with systemic steroids by the neuro-ophthalmic team. Some patients need surgical orbital decompression to allow the optic nerves to breath: here the type of orbital decompression is different from the one described above. The aim is to make room around the
optic nerve at the apex of the orbit
optic nerve at the apex of the orbit

compression of the optic nerve causes papilloedema (swollen optic nerve head) which can lead to loss of vision.
|

this shows the type of apical medial wall orbital decompression that is necessary to make room at the apex of the orbit to decompress optic nerves when there is decrease in vision because of compression.
|
second stage- eye muscle surgery
In thyroid eye disease, scarring can cause permanent damage to the eye muscles. Scar tissue, which forms around muscle fibers, becomes stiff and neither contract’s nor relaxes as easily as the muscle it replaces. The eyes may then become misaligned, causing double vision.
Eye muscle surgery can minimize double vision, but may not completely eliminate it. The goal of this surgery is to create a tunnel of single vision, allowing patients to achieve good straight-ahead vision needed for driving and reading. The patient is able to resume many activities, but still may experience double vision when looking far to the right or left.
Eye muscle surgery can minimize double vision, but may not completely eliminate it. The goal of this surgery is to create a tunnel of single vision, allowing patients to achieve good straight-ahead vision needed for driving and reading. The patient is able to resume many activities, but still may experience double vision when looking far to the right or left.

Strabismus may include deviation of the eye or eyes in any direction and limitation of movement in any direction, often in elevation.
The surgery is performed on an outpatient basis with local anesthesia. In eye muscle surgery, the surgeon repositions the muscles, bringing the eyes into alignment. The incisions are hidden. In approximately 5 to 10 percent of cases, more than one surgery is needed to achieve satisfactory alignment of the eyes. Dr. Patel’s excellent strabismus team will look after this aspect of your thyroid orbitopathy if necessary. Remember, not all patients with
thyroid orbitopathy will need strabismus surgery.
thyroid orbitopathy will need strabismus surgery.
Review of eyelids after
|


Eyelid surgery only with repositioning of the upper and lower eyelids: this helps camouflage the proptosis and also protects the corneas. The cosmetic improvement is also pleasing.
|
Teprotumumab for Thyroid-Associated Ophthalmopathy
Inhibition of the insuling-like growth receptor I (IGF-IR) may be achieved by using various agents called biologics. One in particular, Teprotumumab, is being studied at present in the United States and the FDA has given this drug a “breakthrough” therapy designation.
Teprotumumab is a human monoclonal antibody inhibitor of IGF-IR. This drug is administered intravenously once every three weeks for eight treatments and is only used for those patients who are in the active or inflammatory phase of the disease.
Early results indicate that as many as 69% of patients may show a positive response with a reduction in the proptosis (bulging of the eye) and reduction in the inflammation associated with the active phase of thyroid orbitopathy. This holds great promise as the use of oral or intravenous steroids, whilst certainly useful, give variable results and are also associated with side-effects.
We are awaiting approval by the FDA before we can begin to administer this very promising medication. It is possible that some degree of the effects of thyroid orbitopathy may be partially reversed with this drug. However, as with all things in medicine, one sparrow does not a spring make and we, as clinician scientists, will accurately review results of more than one trial and in more than one country to get an accurate idea of the effectiveness of this medication. Other factors such as side-effects and costs will also have to be considered if approval is obtained. Watch this space!
Teprotumumab is a human monoclonal antibody inhibitor of IGF-IR. This drug is administered intravenously once every three weeks for eight treatments and is only used for those patients who are in the active or inflammatory phase of the disease.
Early results indicate that as many as 69% of patients may show a positive response with a reduction in the proptosis (bulging of the eye) and reduction in the inflammation associated with the active phase of thyroid orbitopathy. This holds great promise as the use of oral or intravenous steroids, whilst certainly useful, give variable results and are also associated with side-effects.
We are awaiting approval by the FDA before we can begin to administer this very promising medication. It is possible that some degree of the effects of thyroid orbitopathy may be partially reversed with this drug. However, as with all things in medicine, one sparrow does not a spring make and we, as clinician scientists, will accurately review results of more than one trial and in more than one country to get an accurate idea of the effectiveness of this medication. Other factors such as side-effects and costs will also have to be considered if approval is obtained. Watch this space!
Prominent Eyes and Eyelid Revision Surgery


Eyelid repositioning to improve corneal protection.
|
Although patients with thyroid ophthalmopathy will have proptosis and upper and lower eyelid retraction, there are other causes of relative prominence of eyes and upper and/or lower eyelid retraction. These include:
|
Customized Treatment
Even when there is eyelid malposition in the absence of thyroid orbitopathy, repositioning of the upper and/or lower eyelids (and sometimes other surrounding structures) may be necessary to protect the corneas. Dr. Patel has designed and published surgical techniques which allow us to improve the protection of the globes in an aesthetically pleasing way. The aim is to protect the corneas, improve the degree of upper and/or lower eyelid retraction (scleral show), reposition the inner and/or outer corner of the eyelids to their proper position and improve dryness and discomfort.
There are times when orbital decompression surgery to reposition the eyeballs posteriorly may be necessary even in the absence of thyroid orbitopathy. However, this is undertaken only after careful consideration of all options.
There are times when orbital decompression surgery to reposition the eyeballs posteriorly may be necessary even in the absence of thyroid orbitopathy. However, this is undertaken only after careful consideration of all options.
Cosmetic Orbital Decompression
Some people have very prominent eyes or asymmetry of the eyes where one is bulging. Often this is caused by a medical condition called Graves’ disease or thyroid eye disease. But often the eyes appear bulgy or prominent due to trauma or just being born that way. This can be quite concerning for many people in that it makes them appear intense or not “normal.” Many patients ask if there is anything that can be done and in the past, the answer
was not too much, at least safely.
Today, this is no longer the case. With advances in the understanding or bony and soft tissue anatomy and the changes one sees in thyroid orbitopathy and other conditions, it is now possible to design a decompression approach which we call “cosmetic orbital decompression.” This is usually undertaken with other soft-tissue work, like on the eyelids,
the cheeks and sometimes the brows.
These are powerful operations which can be quite life changing!
was not too much, at least safely.
Today, this is no longer the case. With advances in the understanding or bony and soft tissue anatomy and the changes one sees in thyroid orbitopathy and other conditions, it is now possible to design a decompression approach which we call “cosmetic orbital decompression.” This is usually undertaken with other soft-tissue work, like on the eyelids,
the cheeks and sometimes the brows.
These are powerful operations which can be quite life changing!
Customized Approach To Surgery
Orbital surgery of any kind should never be undertaken lightly. There is a reason why the majority of plastic surgeons do not undertake this type of surgery: it requires specialist training, detailed knowledge and experience.
First and foremost, when performed in the presence of thyroid orbitopathy, the disease has to be in the non-inflammatory phase and the thyroid control has to have been stable for at least a year.
The degree to which the orbital changes cause problems need to be assessed: these changes may affect you cosmetically, with dryness, redness, irritation or even orbital pain. Examination will show us the degree to which these findings may or may not be helped.
A detailed assessment of a CT scan allows us to assess the soft tissue and bony anatomy and changes. All orbital decompressions are not the same. The old-fashioned traditional “we will remove the floor of your orbit” decompressions are not performed in our clinic as they can be complicated by myriad problems including temporary or permanent double vision, malposition of the eyeball (“sunset syndrome”), permanent numbness, and need for further surgery.
When surgery is planned, we will discuss with you the best approach. Whereas a detailed discussion of the surgical procedure may not be helpful to you, you should be aware that we will be addressing some or all of the following parts of your orbits and face:
This type of surgery surgery is performed under general anesthesia and takes about an hour to two hours, depending upon everything that needs to be done. Patients are allowed home the same day with written instructions. Bruising and swelling are at their worst for the first two weeks: use of ice helps a lot. It should be remembered that some degree of swelling and bruising in patients with thyroid orbitopathy will remain for several weeks.
and patients recover in about two weeks with bruising and swelling. Although the surgery only takes an hour or two to perform, these are complex procedures. We will ensure we discuss your postoperative care, time off work, physical activities, etc with you prior to and after your surgery. Every patient is different and we can only provide you with rough guidelines.
A detailed knowledge of anatomy and physiology are paramount when designing orbital decompressions.
First and foremost, when performed in the presence of thyroid orbitopathy, the disease has to be in the non-inflammatory phase and the thyroid control has to have been stable for at least a year.
The degree to which the orbital changes cause problems need to be assessed: these changes may affect you cosmetically, with dryness, redness, irritation or even orbital pain. Examination will show us the degree to which these findings may or may not be helped.
A detailed assessment of a CT scan allows us to assess the soft tissue and bony anatomy and changes. All orbital decompressions are not the same. The old-fashioned traditional “we will remove the floor of your orbit” decompressions are not performed in our clinic as they can be complicated by myriad problems including temporary or permanent double vision, malposition of the eyeball (“sunset syndrome”), permanent numbness, and need for further surgery.
When surgery is planned, we will discuss with you the best approach. Whereas a detailed discussion of the surgical procedure may not be helpful to you, you should be aware that we will be addressing some or all of the following parts of your orbits and face:
- The bony orbit
- The soft tissue orbit (fat)
- Upper eyelid retractors
- Lower eyelid retractors
- Lateral canthus
- Soft tissue and/or skin excess
- Cheek ptosis
- Negative malar eminence
This type of surgery surgery is performed under general anesthesia and takes about an hour to two hours, depending upon everything that needs to be done. Patients are allowed home the same day with written instructions. Bruising and swelling are at their worst for the first two weeks: use of ice helps a lot. It should be remembered that some degree of swelling and bruising in patients with thyroid orbitopathy will remain for several weeks.
and patients recover in about two weeks with bruising and swelling. Although the surgery only takes an hour or two to perform, these are complex procedures. We will ensure we discuss your postoperative care, time off work, physical activities, etc with you prior to and after your surgery. Every patient is different and we can only provide you with rough guidelines.
A detailed knowledge of anatomy and physiology are paramount when designing orbital decompressions.
|
|
|
|
"I had a excellent eye lift done by Dr. Patel. He knows what he is doing and is very pleasant. Dr.Patel was easy to get an appointment and he works with you. The office staff was very pleasant and made you feel calm." D. Gull Highly recommended for eye lift surgery - Salt Lake City, UT

Visit Patel Plastic Surgery on YouTube for more free tips!
Stay Connected With Us On Social Media
|
Find UsLocations:
Dr. BCK Patel MD, FRCS 1025E 3300S Salt Lake City, Utah 84106, USA (801) 413-3599 (phone/text) E: [email protected] bckpatel.info --------------------------------------- Dr. BCK Patel MD, FRCS 585 E Riverside Dr Suite 201 Saint George, UT 84790 (435) 215-0014 E: [email protected] Quick-Link |
Let Us answer your questions |