For Residents, Fellows, Oncologists, Ophthalmologists, Plastic Surgeons, Dermatologists
Diagnosis, Grading, Treatment, Prognosis

Conjunctival Squamous Neoplasia

Squamous cell carcinoma of the conjunctiva is at the advanced spectrum of ocular surface neoplastic disease termed “ocular surface squamous neoplasia” (OSSN).
Risk factors for OSSN:
- Ultraviolet light
- HIV/AIDS
- Human papilloma virus
- Allergic conjunctivitis
- Smoking
Africa has the highest incidence of OSSN in the world because of the high levels of ultraviolet light radiation and also because of the higher incidence of HIV/AIDS. OSSN affects 1.3 out of 100,000 people per year. This is X10 higher than the incidence elsewhere in the world.
In equatorial Africa, OSSN affects younger adults and proportionately more women are affected than in other parts of the world. The age of presentation in Africa is 40 years compared to 60 years in other parts of the world. In Africa, 2/3rds of the tumors are seen in females whereas 70% are males elsewhere in the world
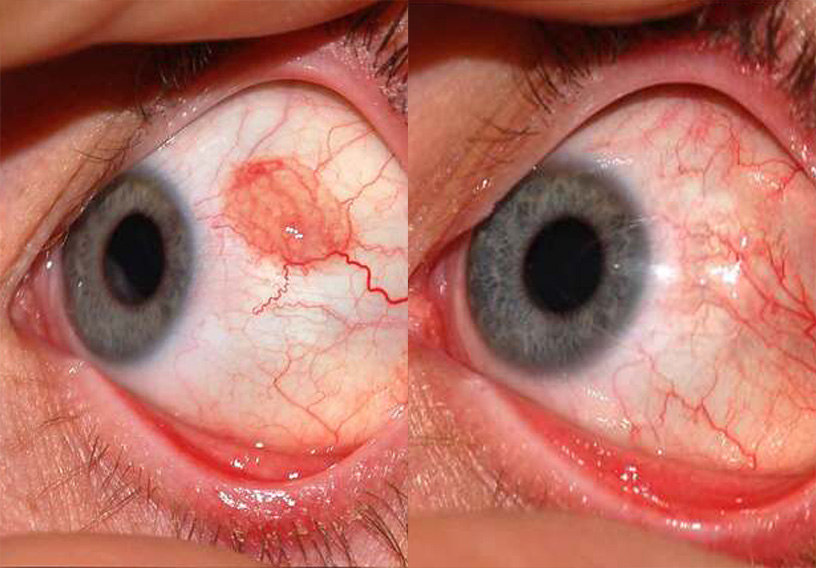
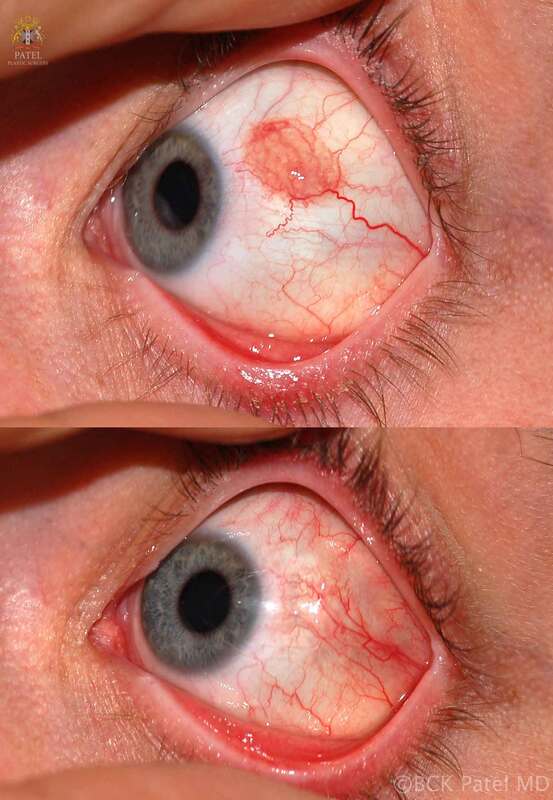
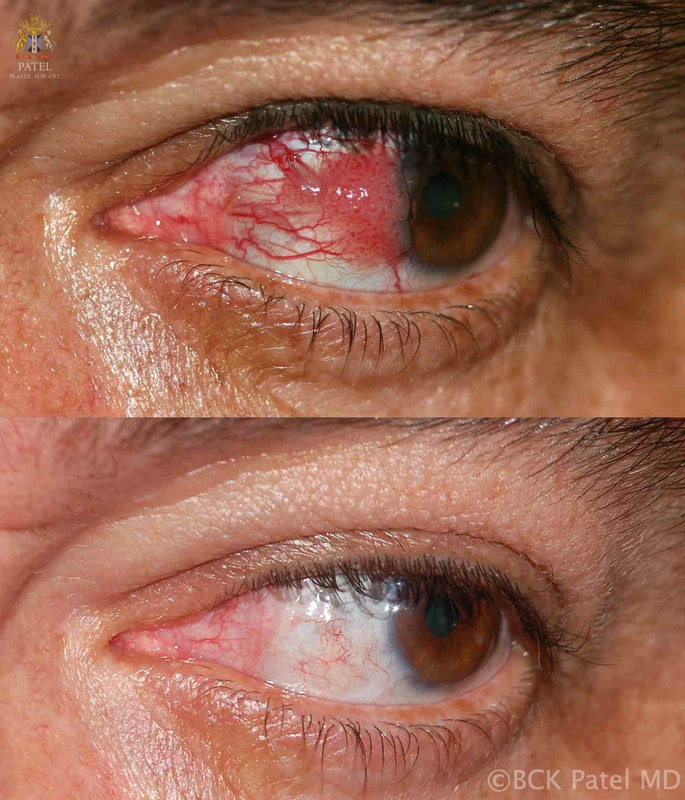
Clinical Presentation
Patients will present with:
- Red Eye
- Photophobia
- Irritation
- Foreign Body Sensation
- Progressive Growth of Conjunctival Lesion
Most of the lesions grow on the nasal conjunctiva in the interpalpebral fissure. The lesions involve the conjunctiva initially and may extend onto the cornea. The lesions will show elevation, a fibrovascular growth with markedly dilated vessels and pigmentation is common in the African population.

Classification of squamous cell carcinoma of the conjunctiva
The classification of conjunctival squamous neoplasia is based upon two main primary tumor characteristics: the degree of the depth of invasion of the tumor, which can only really be assessed by histopathologic evaluation, and the involvement of the surrounding structures such as sclera, cornea, eyelid, orbit, which may be assessed by imaging studies.
Diffuse disease that has not invaded the sclera or the cornea is graded as Tumor In Situ or “TIS”. Further gradation is from T1 to T4 and is based upon the largest basal dimension of the tumour (T1 is less than 5 mm and T2 is more than 5 mm), and the presence of adjacent structure involvement (Stages T3 or T4). This deeper involvement is assessed by clinical examination and imaging studies.
Tumor Staging
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor (≤5 mm in the greatest dimension) invades through the conjunctival basement membrane without invasion of adjacent structures |
| T2 | Tumor (>5 mm in greatest dimension) invades through the conjunctival basement membrane without invasion of adjacent structures |
| T3 | Tumor invades adjacent structures (excluding the orbit) |
| T4 | Tumor invades the orbit with or without further extension |
| T4a | Tumor invades orbital soft tissue without bone invasion |
| T4b | Tumor invades the bone |
| T4c | Tumor invades adjacent paranasal sinuses |
| T4d | Tumor invades the brain |
The T4 category includes all conjunctival tumors with orbital or further extension into bone, sinus, and brain. The T3 category encompasses a wide spectrum of tumors with broad surface extension to the cornea and eyelid and/or deep invasion of the sclera and other intraocular compartments.
Assessment of a patient with squamous cell carcinoma of the conjunctiva
Demographic information should include age, race, sex, laterality of the disease, the immune status of the patient and details of any prior treatments (surgery, drops, irradiation, etc).
Examination: a complete slit-lamp and fundus examination is carried out and the following details are documented:
- Tumor Location
- Largest Base Diameter
- Growth pattern-invasion of surrounding structures (plica semilunaris, caruncle, cornea, sclera, tarsal conjunctiva, fornix conjunctiva, lacrimal punctum, eyelid, intraocular compartments, orbit)
- Measurement of the corneal extension in clock hours
- Palpation of preauricular and submandibular lymph nodes
- Assessment of the orbit (see section on examination of the orbit in our textbook “Orbital Tumors” by Singh and Patel
Documentation:
All tumors should be photographed macroscopically and through the slit-lamp Photographs of both eyes should be taken for comparision purposes
Management OF A PATIENT WITH SQUAMOUS CELL CARCINOMA OF THE CONJUNCTIVA
Excisional Biopsy: when an excisional biopsy is performed, a 2 mm margin is left. When there is corneal extension, the involved corneal epithelium is removed together with a 1-mm border of uninvolved corneal epithelium beyond the visible tumor margin after denaturation with absolute alcohol for one minute.
In cases where scleral invasion is suspected, a partial-thickness scleral flap is created to obtain tumour-free margins.
The conjunctival, limbal, and cornel components of the tumour are excised and submitted as a single piece in formalin for histopathological assessment.
A double freeze-thaw cryotherapy cycle is then applied to the conjunctival margins of the resection.
The conjunctival defect may be closed with primary closure, with the use of a conjunctival autograft, or with amniotic membrane.
When eyelid invasion is suspected, a 2.5-mm punch is used to obtain a sample or samples of the tarsal conjunctiva and tarsus.
Histopathologically, conjunctival sqamous neoplasia is classified as:
- Mild dysplasia (CIN grade 1/3)
- Moderate dysplasia (CIN grae 2/3), severe dysplasia (CIN grade 3/3)
- Invasive squamous cell carcinoma
Treatment Course
Most conjunctival squamous cell carcinomas are treated with complete excision and with the application of cryotherapy.
If there are positive surgical margins, patients are put on local adjuvant therapy which can include interferon (IFN) α−2B injections or drops, fluorouracin (5-FU) 1%, or mitomycin C (MMC 0.04%.
Use of 5FU 1% eye drops applied four times a day for four weeks after the surgical site has healed (about 3 weeks) decreases the risk of recurrence at one year from 36% to 11%.
Patients with scleral invasion may require brachytherapy.
In Africa, all patients presenting with sqamous cell carcinoma of the conjunctiva should be tested for HIV.
Prognosis
When a tumor is removed completely with clear margins, the recurrence is about 10%. When only incisional biopsies are obtained and lesions treated with adjuvant therapy, the recurrence can be as high as 25% over 18 months.
As with all malignant tumors, follow up is necessary. In Africa, reviews are done at one month, three months, six months and a year after surgery. Subsequently, patients are examined at 18 months, 24 months and 36 months after surgery.
Summary
The majority of conjunctival sqamous cell carcinomas are stage Tis (carcinoma in situ) when properly assessed with relevant biopsy.
Topical IFN a 2-B as a primary treatment for diffiuse conjunctival and/pr corneal disease gives excellent outcomes as does the use of this as a postoperative adjuvant therapy when there are positive margins or there is recurrence.
IFN a 2-B has been shown to be as effective as topical chemotherapeutic agents including MMC and 5-FU in achieving tumor regression and is associated with lower complications.
When there is scleral invasion, topical therapy is not recommended. A more effective treatment is the use of brachytherapy. Surface brachytherapy for scleral invasion may avoid the need for an enucleation.
References
- Margo CE, White AA. Ocular surface squamous neoplasia: terminology that is conceptually friendly but clinically perilous. Eye. 2014;28:507–509. [PubMed: 24807632]
- Conway RM, Graue GF, Pelayes DE, et al. Conjunctival Carcinoma. American Joint Committee on Cancer (AJCC) AJCC Cancer Staging Manual 8th ed. New York, NY: Springer; 2017.
- Shields CL, Kaliki S, Kim HJ, et al. Interferon for ocular surface squamous neoplasia in 81 cases: outcomes based on the American Joint Committee on Cancer classification. Cornea. 2013;32:248– 256. [PubMed: 22580436]
- Shah SU, Kaliki S, Kim J, et al. Topical interferon alfa-2b for management of ocular surface squamous neoplasia in 23 cases: outcomes based on American Joint Committee on Cancer Classification. Arch Ophthalmol. 2012;130:159–164. [PubMed: 22332208]
- Galor A, Karp CL, Oellers P, et al. Predictors of ocular surface squamous neoplasia recurrence after excisional surgery. Ophthalmology. 2012;119: 1974–1981. [PubMed: 22704832]
- Kao AA, Galor A, Karp CL, et al. Clinicopathologic correlation of ocular surface squamous neoplasms at Bascom Palmer Eye Institute: 2001 to 2010. Ophthalmology. 2012;119:1773–1776. [PubMed: 22771047]
- Chauhan S, Sen S, Sharma A, et al. American Joint Committee on Cancer Staging and Clinicopathological High-Risk Predictors of Ocular Surface Squamous Neoplasia. Arch Pathol Lab Med. 2014;138:1488–1494. [PubMed: 25357110]
- Nanji AA, Moon CS, Galor A, et al. Surgical versus medical treatment of ocular surface squamous neoplasia: a comparison of recurrences and complications. Ophthalmology. 2014;121:994–1000. [PubMed: 24411578]
- Parrozzani R, Frizziero L, Trainiti S, et al. Topical 1% 5-fluoruracil as a sole treatment of corneoconjunctival ocular surface squamous neoplasia: long-term study. Br J Ophthalmol. 2017;101:1094–1099. [PubMed: 27941046]
- Yousef YA, Finger PT. Squamous carcinoma and dysplasia of the conjunctiva and cornea. Ophthalmology. 2012;119:233–240. [PubMed: 22189448]
- Zarei-Ghanavati S, Alizadeh R, Deng SX. Topical interferon alpha-2b for treatment of noninvasive ocular surface squamous neoplasia with 360 degrees limbal involvement. J Ophthalmic Vis Res 2014;9:423–426. [PubMed: 25709765]
- Sturges A, Butt AL, Lai JE, et al. Topical interferon or surgical excision for the management of primary ocular surface squamous neoplasia. Ophthalmology. 2008;115:1297–1302. [PubMed:18294690]
- Kim HJ, Shields CL, Shah SU, et al. Giant ocular surface squamous neoplasia neoplasia managed with interferon alpha-2b as immunotherapy or immunoreduction. Ophthalmology. 2012;119:938–944. [PubMed: 22361315]
- Schechter BA, Koreishi AF, Karp CL, et al. Long-term follow-up of conjunctival and corneal intraepithelial neoplasia treated with topical interferon alfa-2b. Ophthalmology. 2008;115:1291–1296. [PubMed: 18187195]
- Karp CL, Moore JK, Rosa RH, Jr. Treatment of conjunctival and corneal intraepithelial neoplasia with topical interferon alpha-2b. Ophthalmology. 2001;108:1093–1098. [PubMed: 11382635]
- Boehm MD, Huang AJ. Treatment of recurrent corneal and conjunctival intraepithelial neoplasia with topical interferon alfa 2b. Ophthalmology. 2004;111:1755–1761. [PubMed: 15350333]
- Poothullil AM, Colby KA. Topical medical therapies for ocular surface tumors. Semin Ophthalmol. 2006;21:161–169. [PubMed: 16912014]
- Galor A, Karp CL, Chhabra S, et al. Topical interferon alpha 2b eye-drops for treatment of ocular surface squamous neoplasia: a dose comparison study. Br J Ophthalmol. 2010;94:551–554. [PubMed: 19493859]
- Huerva V, Mangues I. Treatment of conjunctival squamous neoplasias with interferon alpha 2b. J Fr Ophtalmol. 2008;31:317–325. [PubMed: 18404128]
- Aronow ME, Singh AD. Radiation therapy: conjunctival and eyelid tumors. Dev Ophthalmol. 2013;52:85–93. [PubMed: 23989129]
- Arepalli S, Kaliki S, Shields CL, et al. Plaque radiotherapy in the management of scleral-invasive conjunctival squamous cell carcinoma. JAMA Ophthalmol. 2014;132:691–696. [PubMed: 24557333]
- Graue GF, Tena LB, Finger PT. Electron beam radiation for conjunctival squamous carcinoma. Ophthal Plast Reconstr Surg. 2011;27: 277–281.
- Gichuhi S, Sagoo MS. Squamous cell carcinoma of the conjunctiva Community Eye Health 2016;29(95):52-53